

Socioeconomic profile and vulnerabilities of people receiving home-based palliative care in Kerala, India
- PMID: 40604810
- PMCID: PMC12220499
- DOI: 10.1186/s12904-025-01834-y
Socioeconomic profile and vulnerabilities of people receiving home-based palliative care in Kerala, India
Abstract
Introduction: Home-based palliative care (HBPC) enhances access to palliative care, reduces health-related costs, and improves health outcomes. However, studies centered on the socioeconomic profile of HBPC are limited. This study aimed to describe the socio-economic profile of HBPC recipients in Kerala, India, and to assess the impact of the disease on the financial, educational, and employment status of their family members.
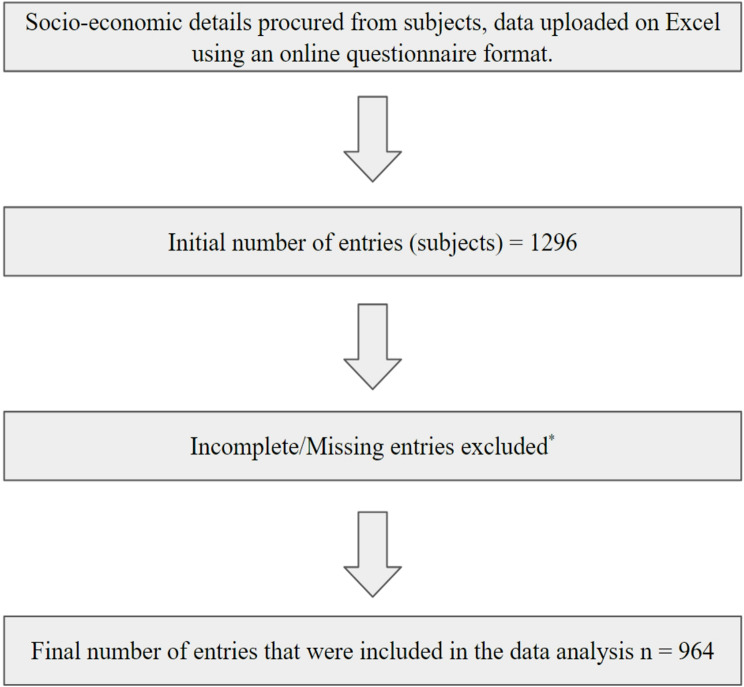
Methods: The socio-economic details of HBPC beneficiaries of a non-profit palliative care organization were collected. Individuals enrolled under HBPC who first received it between March 2020 and April 2024 were included in this study. Data on the socioeconomic details of the beneficiaries were extracted and digitized from registries maintained by Pallium India. Of the 1296 entries received, 964 with complete data were included in the final analysis, which was performed using Jamovi v2.3.28.
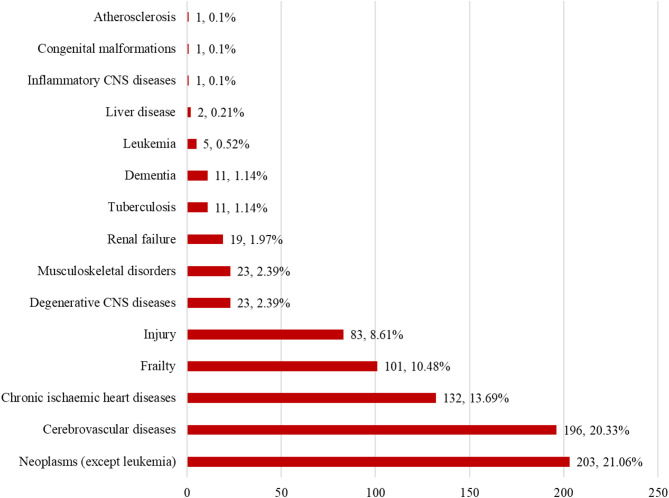
Results: The mean (SD) age of the beneficiaries was 61.0 (16.6) years. Among the total, 52.9% of the beneficiaries were female, and the median (IQR) family size was 9 (6-13). A total of 83.25% lived in their own homes, and 62.97% resided in rural areas. Cancer (21.1%), followed by Cerebrovascular diseases (20.3%), were the two most common conditions requiring HBPC. Debt was reported by 31.3% of families, with a median (IQR) debt of 2389.5 (597.4-4779.0) USD. The primary reason for debt was health-related expenses. 62.5% of families had beneficiaries receiving pensions, and 7.21% received support from another organization. In 4.2% of families, there was no breadwinner, and 9.5% and 66.8% of patients could not afford food and medicines, respectively. A family member lost their job in 8.0% of families, while in 2.8% of families, a child had to discontinue their education due to the patient's illness.
Conclusion: Healthcare costs were the major cause of debt, with many HBPC recipients unable to afford medicines. Moreover, the employment and education of other family members were also threatened. Further strengthening of social and economic security measures is essential to safeguard these individuals and their families.
Keywords: Access to healthcare; Palliative care; Palliative medicine; Public health; Social security.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Institutional Ethics Committee (IEC) of Trivandrum Institute of Palliative Sciences and a waiver for consent was obtained vide reference no: TIPS/IEC-5/2024Exm since the study was a retrospective analysis of medical records. The study was conducted in compliance with the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Anagnostou D. Palliative care improves quality of life and reduces symptom burden in adults with life-limiting illness. Evid Based Nurs. 2017;20(2):47. - PubMed
-
- WHO guidelines for the pharmacological. And radiotherapeutic management of cancer pain in adults and adolescents. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO. - PubMed
-
- Viswanath V, Rao S. Advances in palliative care in 2020: palliative care and oncology in India - Looking ahead from 2020. Indian J Cancer. 2021;58(1):45. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
