

Childhood necrotising pneumonia, empyema and complicated parapneumonic effusion secondary to community acquired pneumonia: report of 158 cases from a tertiary hospital in Egypt
- PMID: 40604976
- PMCID: PMC12224481
- DOI: 10.1186/s12931-025-03291-w
Childhood necrotising pneumonia, empyema and complicated parapneumonic effusion secondary to community acquired pneumonia: report of 158 cases from a tertiary hospital in Egypt
Abstract
Background: Incidence of childhood complicated community acquired pneumonia (cCAP) is increasing worldwide. Necrotising pneumonia (NP), empyema and complicated parapneumonic effusion (CPPE) are the most common local complications.
Methods: This retrospective observational study describes clinical characteristics, aetiology and management of children hospitalized with cCAP in one of the largest tertiary centers in Egypt, over 5 years (December 2017 till September 2022).
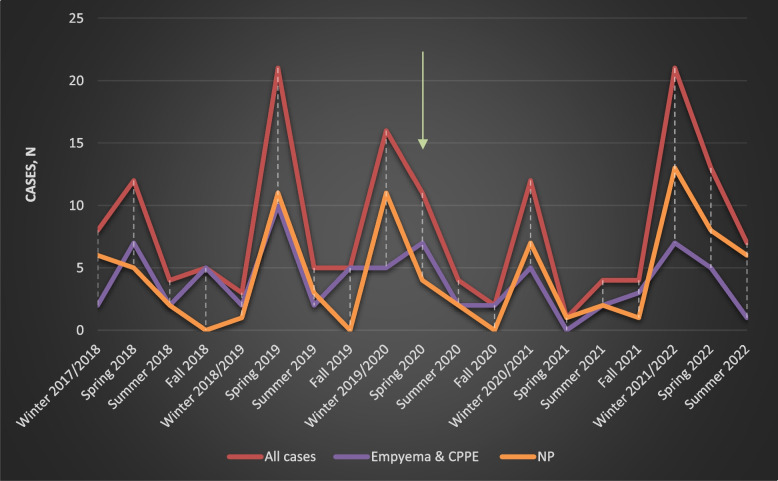
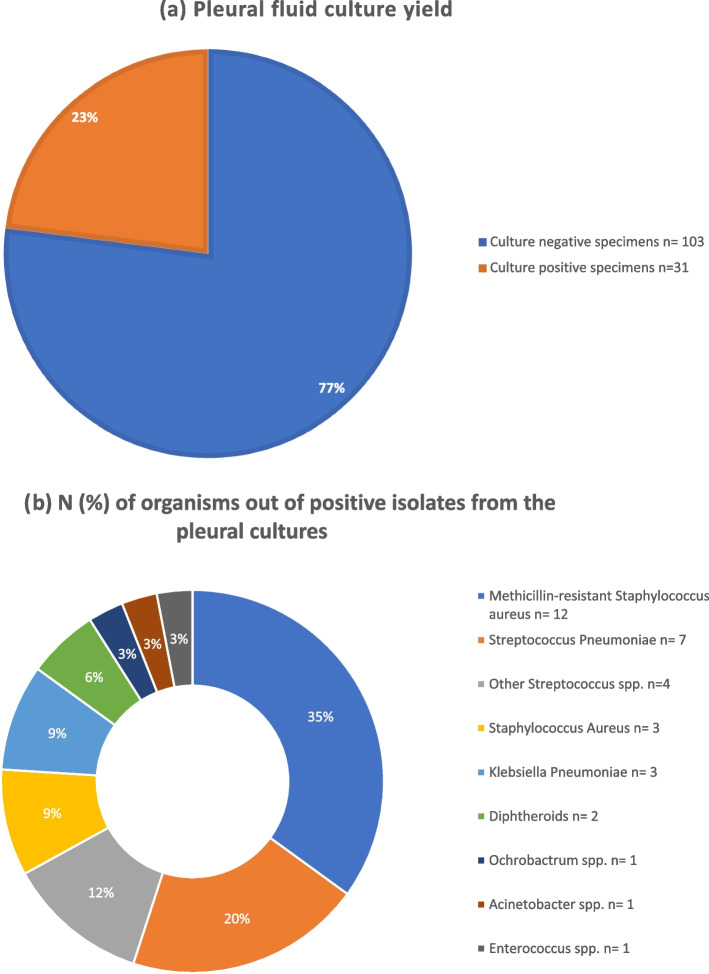
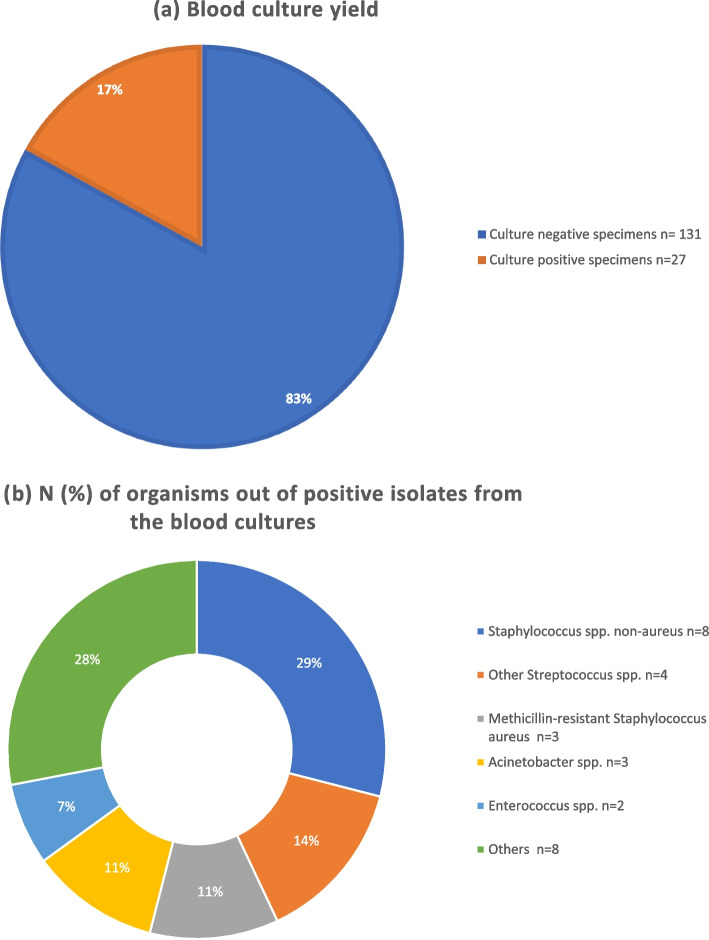
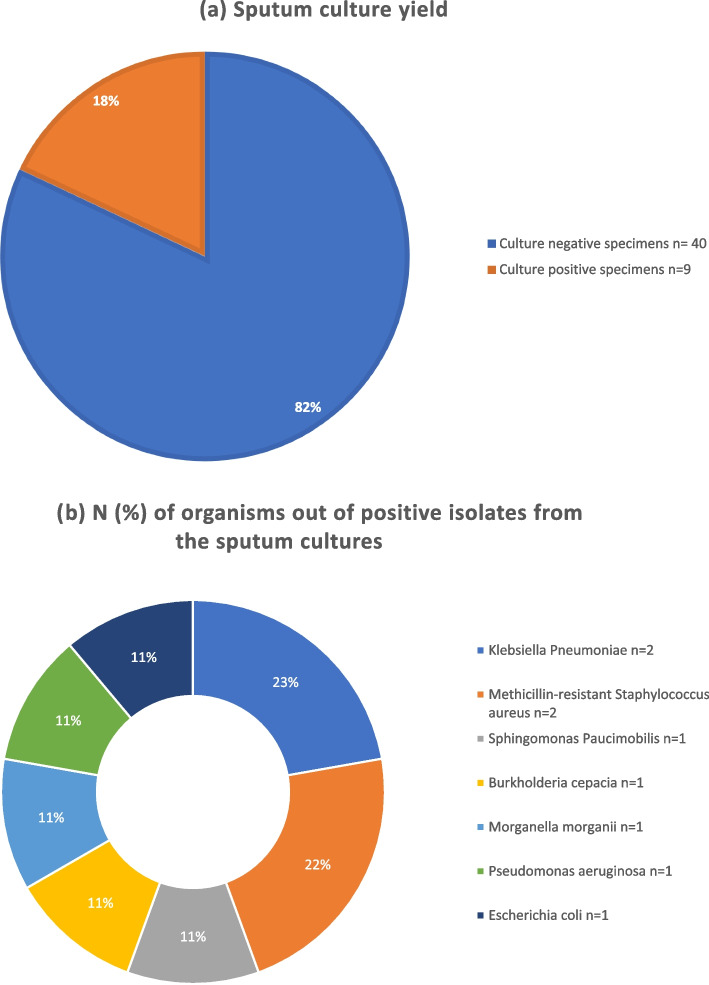
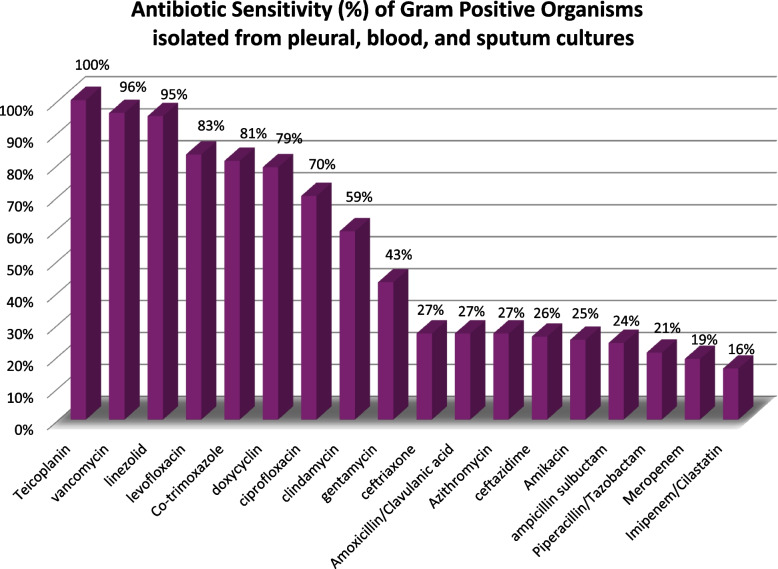
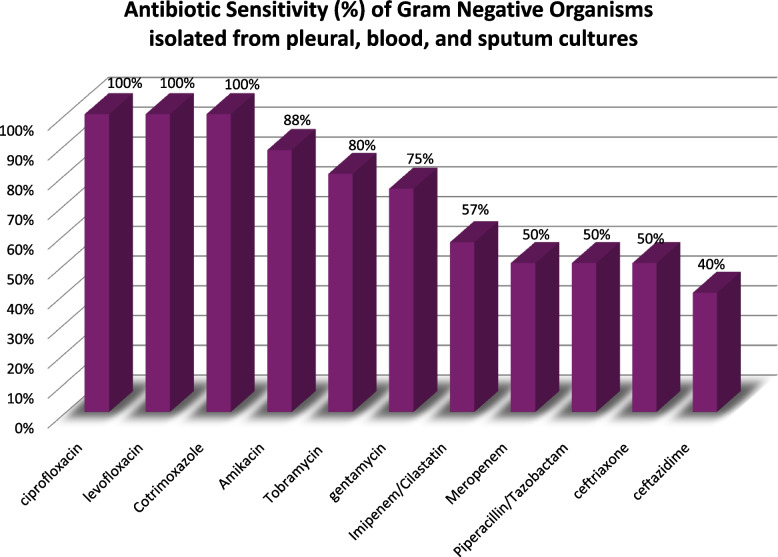
Results: A total of 158 cases were identified. Seasonal variation was observed, as more cases were hospitalized during Winter and Spring. NP, empyema and CPPE, were diagnosed in 85 (54%), 52 (33%) and 21 (13%) children, respectively. 54 (64%) of children presented with NP had associated empyema or CPPE. The yield of pleural fluid, sputum and blood cultures were 23%, 18% and 17%, respectively. Community acquired MRSA was the predominant causative organism, followed by S pneumoniae. 87% of the patients had pleural interventions. 29 (18%) children received fibrinolytics. Three children presented with CAP and highly septated effusion, developed NP and persistent air leaks following fibrinolytic administration. Patients had prolonged hospitalization (median 17 days). 15 (10%) children had surgery. Children presented with NP had more morbidities and longer length of hospital stay, compared to children presented with CPPE and empyema. ICU admission, mechanical ventilation, severe anemia requiring blood transfusion, broncho-pleural fistula and surgical interventions were significantly higher in NP cohort. We report 5 mortalities, 4 of them below 1 year of age.
Conclusions: This study describes the largest cohort of children hospitalized with cCAP from Egypt till this date. Management of cCAP remains challenging worldwide and the current guidelines requires updating. Improvement of microbial detection and reporting is needed to promote antimicrobial stewardship.
Keywords: COVID-19; Children; Community acquired pneumonia; Complicated pneumonia; Empyema; Necrotising pneumonia; Necrotizing pneumonia; Parapneumonic effusion; Pleural effusion; Pleural fibrinolytics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study protocol was reviewed and approved by the Research Ethics Committee of faculty of medicie- Ain Shams University (R252/2023). The study was approved by the ethical committee of Ain Shams University hospitals. FWA number 000017585. The requirement for informed consent was waived due to the retrospective nature of the study. Consent for publication: Written informed consent was not required because of the retrospective nature for this study. Competing interests: The authors declare no competing interests.
Figures
References
-
- Roeger C, Blacker B, Khalil IA, Rao PC, Cao J, Zimsen SR, et al. GBD 2016 Lower Respiratory Infections Collaborators Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–210. - DOI - PMC - PubMed
-
- Bender RG, Sirota SB, Swetschinski LR, Dominguez RM, Novotney A, Wool EE, et al. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2024;24(9):974–1002. - DOI - PMC - PubMed
-
- Hussien SM, Hamed T, Mohamed MH, Rashad MM, Elnady HG, Metwally HM, et al. Diagnosis, treatment, and prevention of community-acquired pneumonia in children: an evidence-based clinical practice guideline adapted for the use in Egypt using ‘Adapted ADAPTE.’ Bull Natl Res Centre. 2023;47(1):169. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
