

Prognostic implication of venoarterial extracorporeal membrane oxygenation in acute myocardial infarction-related cardiogenic shock
- PMID: 40605095
- PMCID: PMC12219146
- DOI: 10.1186/s40560-025-00807-w
Prognostic implication of venoarterial extracorporeal membrane oxygenation in acute myocardial infarction-related cardiogenic shock
Abstract
Background: Given the conflicting results regarding the clinical outcomes of venoarterial extracorporeal membrane oxygenation (VA-ECMO) based on etiology, its benefit for patients with cardiogenic shock (CS) remains controversial. This study aimed to report the real-world clinical outcomes of VA-ECMO treatment for patients with CS, based on the presence of acute myocardial infarction (AMI).
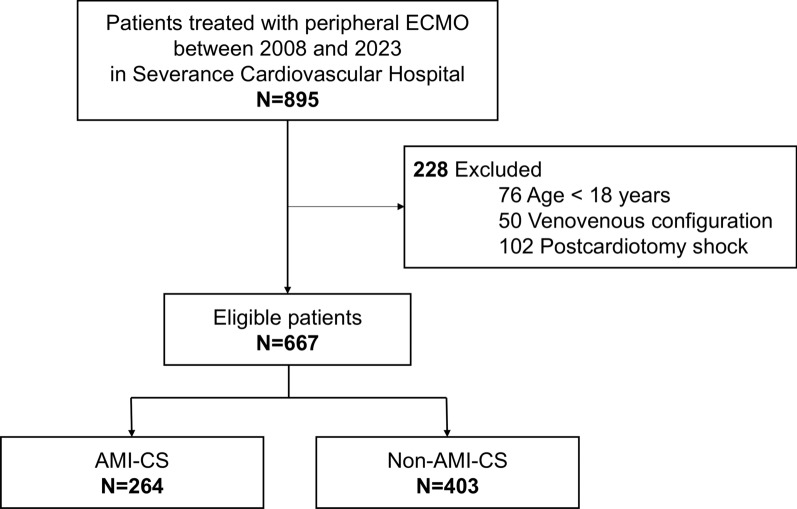
Methods: Patients treated with peripheral VA-ECMO between 2008 and 2023 at a tertiary cardiovascular center were included and classified into two groups based on CS etiology (AMI-CS and non-AMI-CS). Logistic regression models were used to compare in-hospital mortality and to identify prognostic predictors.
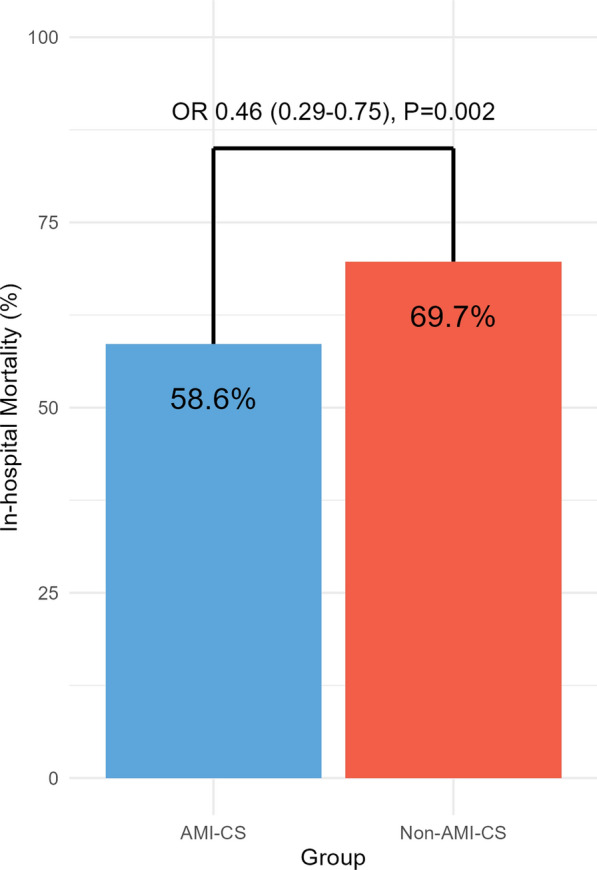
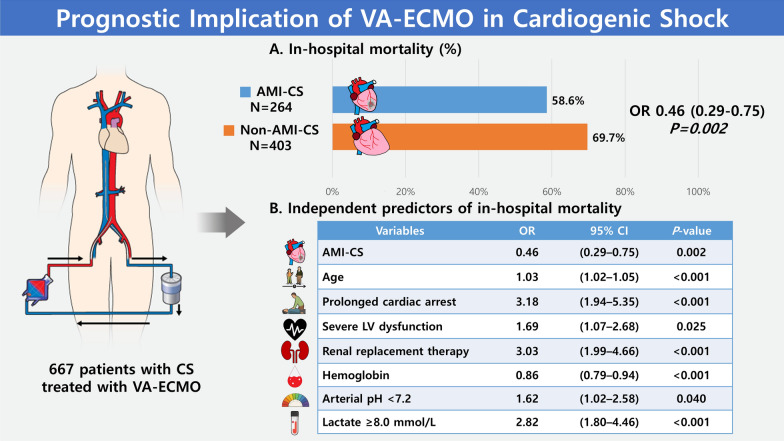
Results: Among the 667 patients included, 264 (39.6%) were classified as having AMI-CS. The rate of cardiac arrest before VA-ECMO initiation was higher in the AMI-CS group than in the non-AMI-CS group (69.7% vs. 55.8%; P < 0.001). Patients in the AMI-CS group were older (66 vs. 61 years; P < 0.001), more likely to be male (82.6% vs. 57.3%; P < 0.001), and had a lower left ventricular (LV) ejection fraction (20% vs. 25%; P < 0.001) than those in the non-AMI-CS group. The AMI-CS group had a lower in-hospital mortality rate (58.6% vs. 69.7%; odds ratio, 0.46; 95% confidence interval, 0.29-0.75; P = 0.002) compared with the non-AMI-CS group. The independent predictors of favorable clinical outcomes after VA-ECMO included younger age, shorter cardiac arrest duration, absence of severe LV dysfunction, absence of renal replacement therapy, higher hemoglobin levels, higher arterial pH, and lower lactate levels. The association between in-hospital mortality and AMI-CS was also demonstrated in the propensity score matching analysis.
Conclusions: In this single-center study, AMI-CS was associated with a lower in-hospital mortality than non-AMI-CS after VA-ECMO treatment.
Keywords: Cardiac arrest; Cardiogenic shock; Extracorporeal membrane oxygenation; Lactate.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Institutional Review Board of Yonsei University and was performed in accordance with the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of this study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Naidu SS, Baran DA, Jentzer JC, Hollenberg SM, van Diepen S, Basir MB, et al. SCAI SHOCK Stage Classification Expert Consensus Update: A Review and Incorporation of Validation Studies: this statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J Am Coll Cardiol. 2022;79(9):933–46. - PubMed
-
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287–96. - PubMed
-
- Thiele H, Akin I, Sandri M, Fuernau G, de Waha S, Meyer-Saraei R, et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med. 2017;377(25):2419–32. - PubMed
-
- Guglin M, Zucker MJ, Bazan VM, Bozkurt B, El Banayosy A, Estep JD, et al. Venoarterial ECMO for adults: JACC scientific expert panel. J Am Coll Cardiol. 2019;73(6):698–716. - PubMed
LinkOut - more resources
Full Text Sources
