

Efficacy and safety of remimazolam combined with remifentanil for sedation during awake fiberoptic intubation: a randomized controlled trial
- PMID: 40605581
- PMCID: PMC12231321
- DOI: 10.1080/07853890.2025.2527951
Efficacy and safety of remimazolam combined with remifentanil for sedation during awake fiberoptic intubation: a randomized controlled trial
Abstract
Introduction: There has been not study determining if remimazolam combined with remifentanil is the reasonable dosing regimen for sedation during awake fiberoptic intubation (AFOI). This prospective double-blind randomized controlled trial compare efficacy and safety of sedation using different-dose remimazolam combined with remifentanil for AFOI procedure.
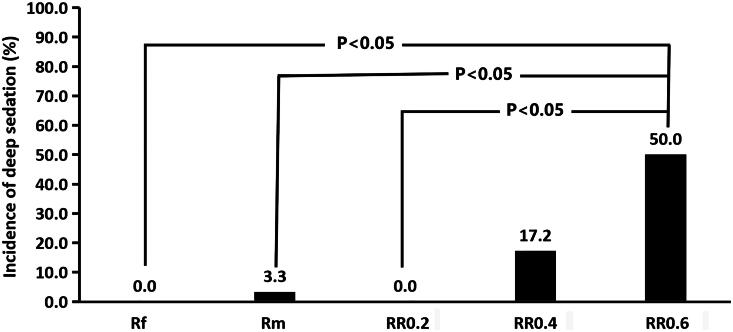
Method: One hundred and fifty patients were randomly assigned to five groups receiving different interventions. The Rf group received only remifentanil infusion of 0.05 mcg/kg/min, the Rm group received only remimazolam 0.6 mg/kg/h, and the RR0.2, RR0.4 and RR0.6 groups received remifentanil 0.05 mcg/kg/min combined with remimazolam of 0.2, 0.4 and 0.6 mg/kg/h, respectively. After intravenous infusion of studied drugs for 3 min, AFOI was carried out under airway topical anesthesia. The primary outcome was the incidence of deep sedation during AFOI procedure.
Results: Deep sedation occurred only in the Rm, RR0.4 and RR0.6 groups, with incidences of 3.3%, 17.2%, and 50.0%, respectively (p < 0.001). The incidence of deep sedation in the RR0.6 group was not statistically different from that in the RR0.4 group (p > 0.05), but was higher than these in the Rf, Rm and RR0.2 groups (p < 0.05). Hypoxemia was observed only in RR0.2, RR0.4 and RR0.6 groups, with incidences of 13.3%, 44.8%, and 44.8%, respectively (p < 0.001). The recall score for AFOI procedure was significantly lower in the four remimazolam groups than in the Rf group (p < 0.005). The patients' reaction score to AFOI procedure, cough severity, incidence of tachycardia, and willingness to repeat the procedure were lower in the RR0.6 group than in the Rf and Rm groups (p < 0.005).
Conclusions: Remimazolam 0.2-0.6 mg/kg/h combined with remifentanil 0.05 mcg/kg/min are effective and feasible dosing regimens of sedation for AFOI procedure in patients with normal airway, but the regimen including remimazolam 0.2 mg/kg/h should be the better choice for balancing efficacy and safety.
Trial registration: Chinese Clinical Trial Registry, ChiCTR2100042917. Retrieved from http://www.chictr.org.cn/showproj.html?proj=65332 on January 31, 2021.
Keywords: Awake fiberoptic intubation; moderate sedation; remifentanil; remimazolam.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources