

Manganese-enhanced MRI during remotely induced myocardial ischemia reperfusion injury in male mice
- PMID: 40605594
- PMCID: PMC12223404
- DOI: 10.14814/phy2.70442
Manganese-enhanced MRI during remotely induced myocardial ischemia reperfusion injury in male mice
Abstract
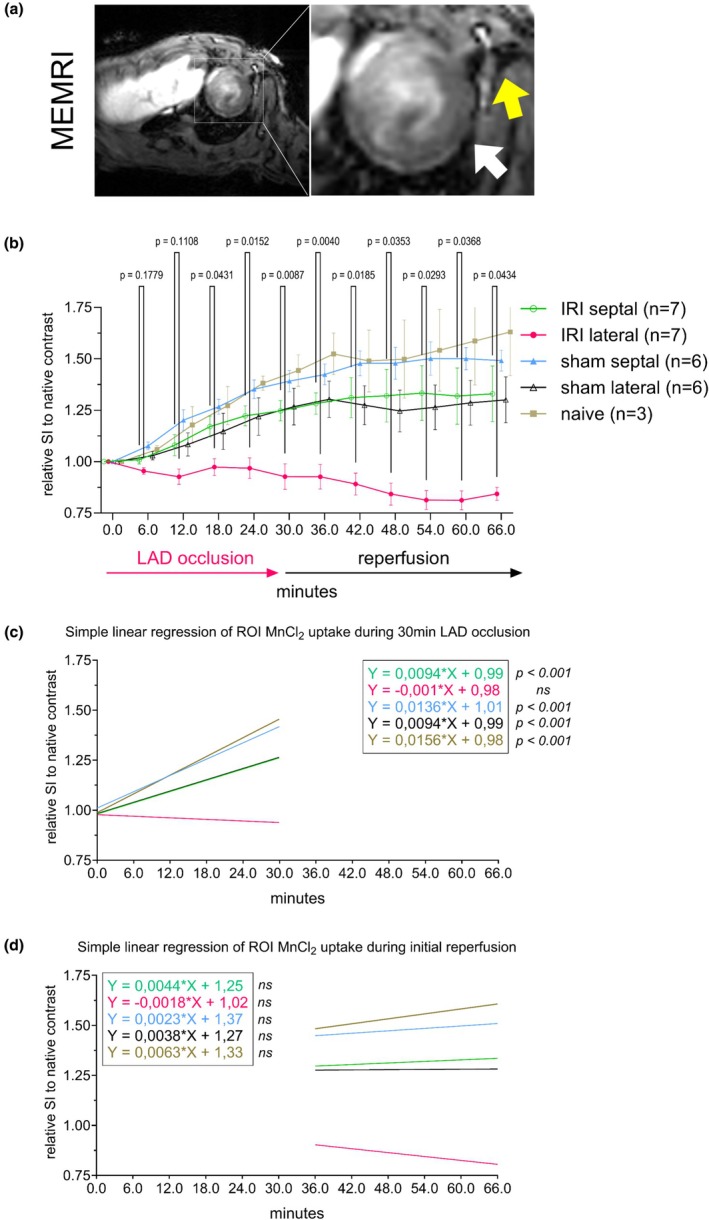
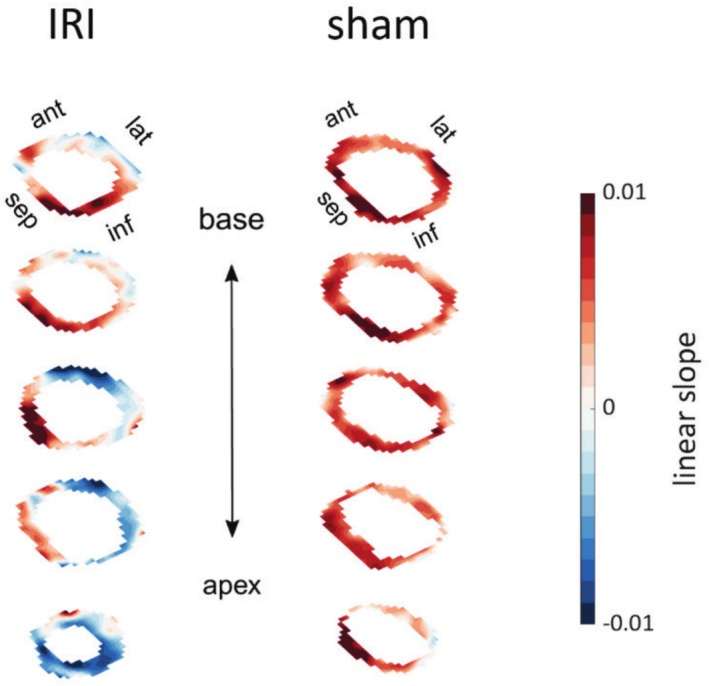
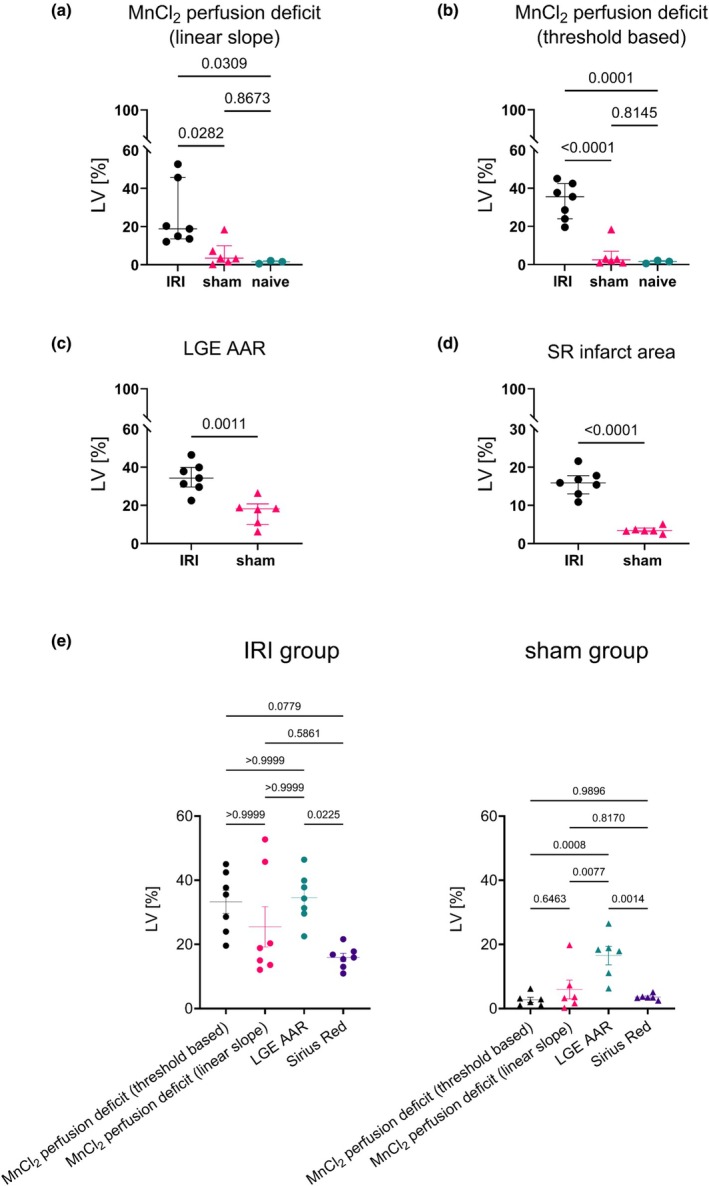
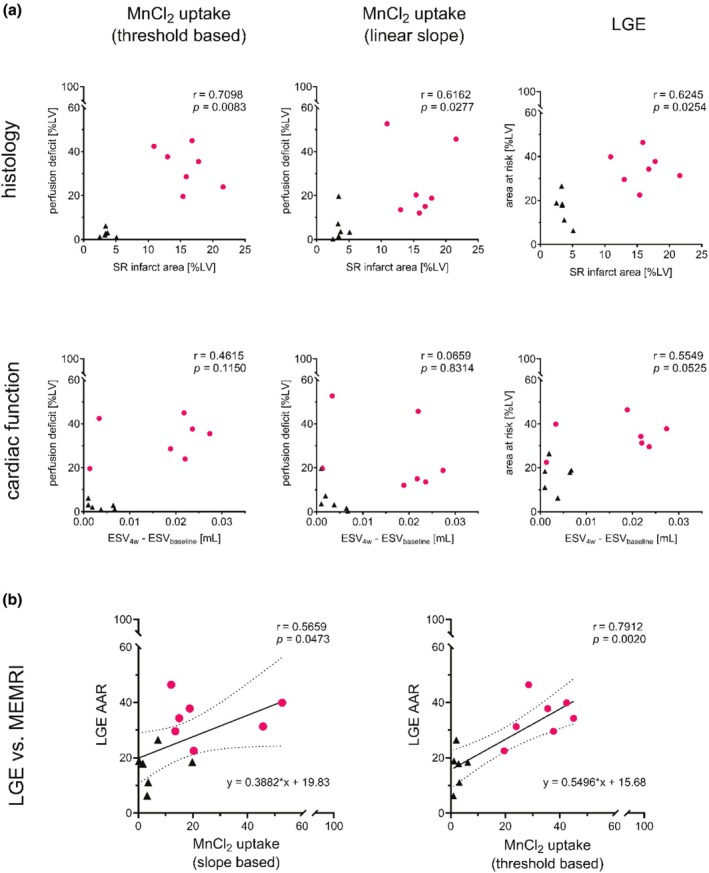
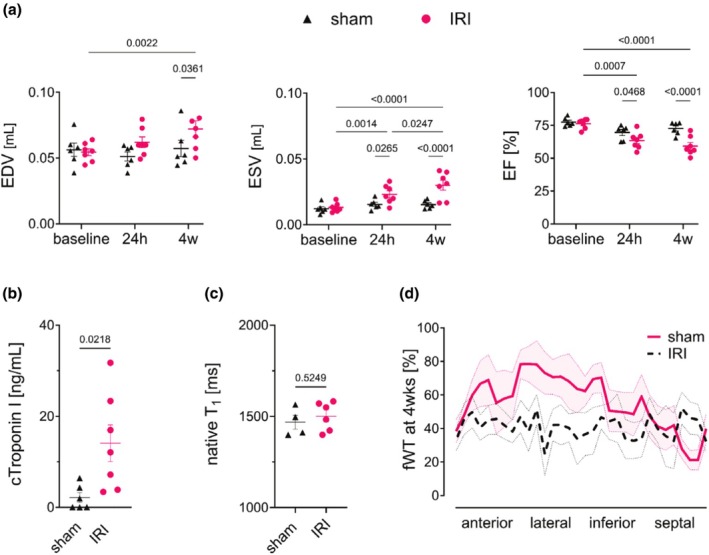
Early assessment of myocardial viability post-ischemia is crucial to mitigate adverse remodeling and optimize therapy. Current noninvasive methods like late gadolinium enhancement (LGE) MRI may overestimate infarct size. Manganese-enhanced MRI (MEMRI) emerged as a promising alternative, offering greater specificity in assessing myocardial damage. We evaluated MEMRI alongside LGE and histology in a murine ischemia-reperfusion model using a novel "in-scanner" remote occlusion technique for real-time imaging during acute ischemia. Male C57BL/6 mice (n = 16) underwent left anterior descending artery occlusion (n = 7), sham surgery (n = 6), or no intervention (n = 3). MEMRI (0.1 mmol/kg MnCl2) during ischemia (0-60 min) and LGE (0.1 mmol/kg Gd-DOTA, 24 h post-surgery) quantified perfusion deficits and infarct size. MEMRI detected acute hypo-perfusion (lateral wall signal reduction: p < 0.01 vs. septal), confined to the occluded territory, while LGE overestimated infarct size (p = 0.0225 vs. histology). Ischemic mice showed adverse remodeling with reduced ejection fraction (61.37% vs. 71.92%, p < 0.01). MEMRI-derived perfusion deficits correlated with functional decline and histology-confirmed infarcts. Pre-occlusion T1 times did not differ between ischemic and sham groups (p = 0.85), confirming technique specificity. MEMRI enables early, accurate ischemic injury detection and predicts cardiac dysfunction, outperforming LGE in infarct size determination. Our remote occlusion technique facilitates real-time perfusion assessments, enhancing preclinical myocardial ischemia studies.
Keywords: ischemia–reperfusion injury; left anterior descending artery; manganese enhanced magnetic resonance imaging; myocardial perfusion; myocardial remodeling.
© 2025 The Author(s). Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Conflict of interest statement
Authors declare no conflict of interest.
Figures
Similar articles
-
Cardiac MRI of differing ischemia and reperfusion times in a myocardial infarction pig model.Sci Rep. 2025 Jul 19;15(1):26270. doi: 10.1038/s41598-025-11390-3. Sci Rep. 2025. PMID: 40683945 Free PMC article.
-
Macro- and microinjury define the heart failure progression after permanent coronary ligation or ischemia-reperfusion in young healthy mice.Am J Physiol Heart Circ Physiol. 2025 Aug 1;329(2):H521-H533. doi: 10.1152/ajpheart.00267.2025. Epub 2025 Jul 16. Am J Physiol Heart Circ Physiol. 2025. PMID: 40668645
-
Dual manganese-enhanced and delayed gadolinium-enhanced MRI detects myocardial border zone injury in a pig ischemia-reperfusion model.Circ Cardiovasc Imaging. 2011 Sep;4(5):574-82. doi: 10.1161/CIRCIMAGING.110.960591. Epub 2011 Jun 30. Circ Cardiovasc Imaging. 2011. PMID: 21719779 Free PMC article.
-
Remote Ischemic Perconditioning to Reduce Reperfusion Injury During Acute ST-Segment-Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2017 May 17;6(5):e005522. doi: 10.1161/JAHA.117.005522. J Am Heart Assoc. 2017. PMID: 28515120 Free PMC article.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
References
-
- Algoet, M. , Pusovnik, M. , Gillijns, H. , Mestdagh, S. , Billiau, J. , Artoos, I. , Gsell, W. , Janssens, S. P. , Himmelreich, U. , & Oosterlinck, W. (2024). Remotely triggered LAD occlusion using a balloon catheter in spontaneously breathing mice. Journal of Visualized Experiments, 205, e66386. 10.3791/66386 - DOI - PubMed
-
- Bulluck, H. , Dharmakumar, R. , Arai, A. E. , Berry, C. , & Hausenloy, D. J. (2018). Cardiovascular magnetic resonance in acute ST‐segment‐elevation myocardial infarction: Recent advances, controversies, and future directions. Circulation, 137, 1949–1964. 10.1161/CIRCULATIONAHA.117.030693 - DOI - PMC - PubMed
-
- Chunming, L. (2025). MRI segmentation and bias field correction. https://www.mathworks.com/matlabcentral/fileexchange/59752‐mri‐segmentat... [24 Aug. 2023]
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
