

Sizing in lung transplantation: principles, practices and ideas for the future
- PMID: 40606298
- PMCID: PMC12221432
- DOI: 10.1016/j.jhlto.2025.100304
Sizing in lung transplantation: principles, practices and ideas for the future
Abstract
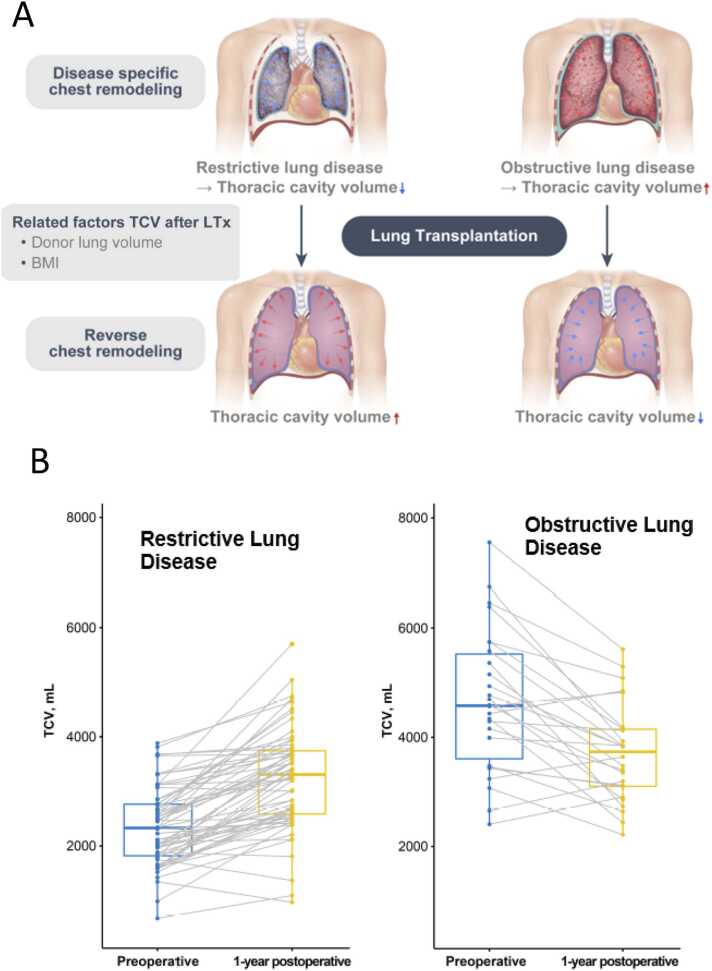
Lung transplantation (LTx) is an important treatment option for many end-stage lung diseases. The goal of LTx is to restore pulmonary physiology (gas exchange and respiratory system mechanics) towards normal, so that LTx recipients can experience an improved quality of life and live significantly longer. An optimized approach to donor-to-recipient size matching is a strategy to increase opportunities for successful transplants and optimize outcomes. In this review we discuss relevant pulmonary gas exchange and respiratory systems mechanics principles as a framework to optimize donor-to-recipient size matching and LTX-recipient management. The predicted total lung capacity (pTLC) is a refined estimate of organ size utilizing regression equations to calculate lung size based on height, sex and age. In general, irrespective of the underlying lung disease the chest cavity is "reverse remolding" back towards normal size in most recipients. The parameter that can reflect the sizing goal to restore physiology towards normal is the recipient pTLC. A pragmatic size matching metric is the donor-to-recipient pTLC-ratio. Significant undersizing based on the pTLC-ratio is a risk factor for complications and lower LTx survival. If significant changes to the LTx candidate's chest cavity size occur (as can occur in severe restrictive lung disease or severe emphysema), or if the chest cavity cannot "reverse remodel" towards normal, it is important to consider additional donor-to-recipient sizing metrics. In addition to the recipient's measured actual total lung capacity imaging-based metrics can be considered. Chest X-ray and computer tomography based volumetric analyses can provide information facilitating a successful LTx.
Keywords: Donor; Lung physiology; Lung transplantation; Matching; Sizing.
© 2025 The Authors.
Conflict of interest statement
The authors have no conflicts to declare.
Figures







References
-
- 〈https://optn.transplant.hrsa.gov/media/nwrksrgl/exec_2024–2027-strategi... (accessed 2/12/25).
Publication types
LinkOut - more resources
Full Text Sources
