

Value of dual-energy computed tomography quantitative parameters in differentiating neoplastic from bland portal vein thrombosis
- PMID: 40606321
- PMCID: PMC12209630
- DOI: 10.21037/qims-2024-2516
Value of dual-energy computed tomography quantitative parameters in differentiating neoplastic from bland portal vein thrombosis
Abstract
Background: Portal vein thrombosis (PVT) is a common clinical pathological state involving distinct pathophysiological processes. Accurate discrimination of PVT nature is of utmost importance for guiding treatment strategies, but histopathology has limitations and imaging lacks quantitative indices. This study aimed to evaluate the feasibility and diagnostic value of quantitative parameters from dual-energy computed tomography (DECT), an advanced technique that allows for such quantitative evaluation, in distinguishing neoplastic from bland PVT.
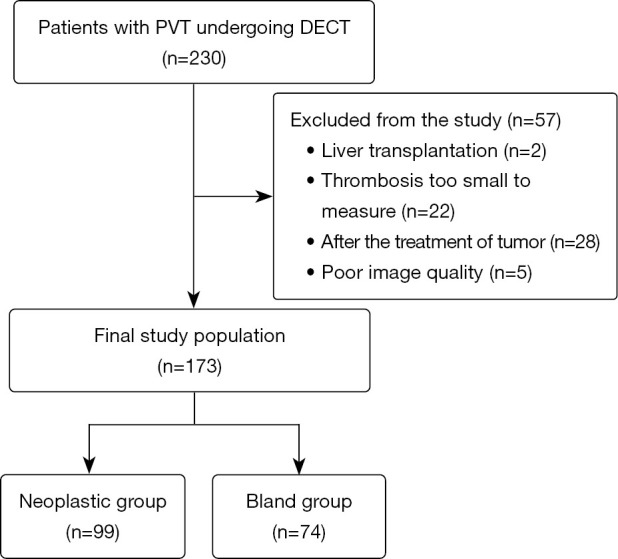
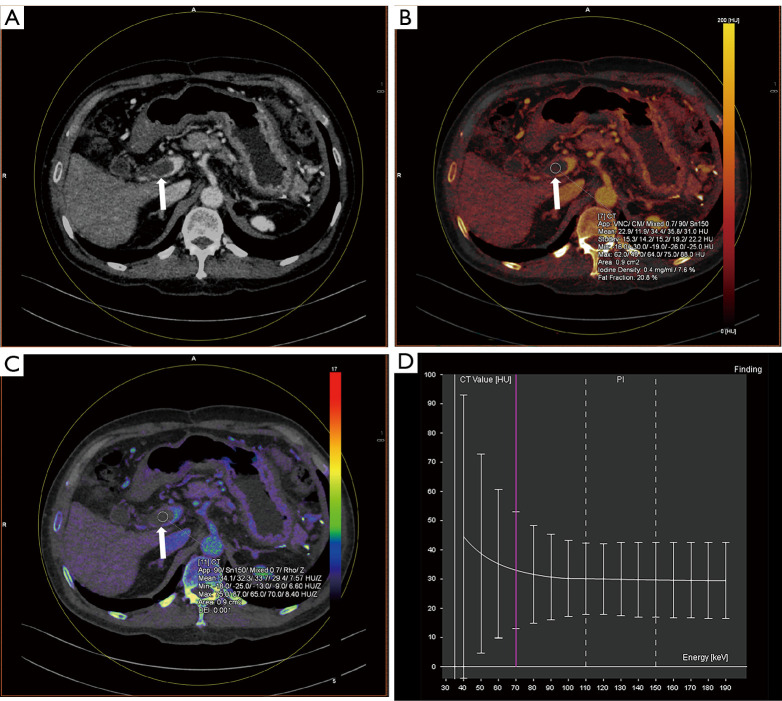
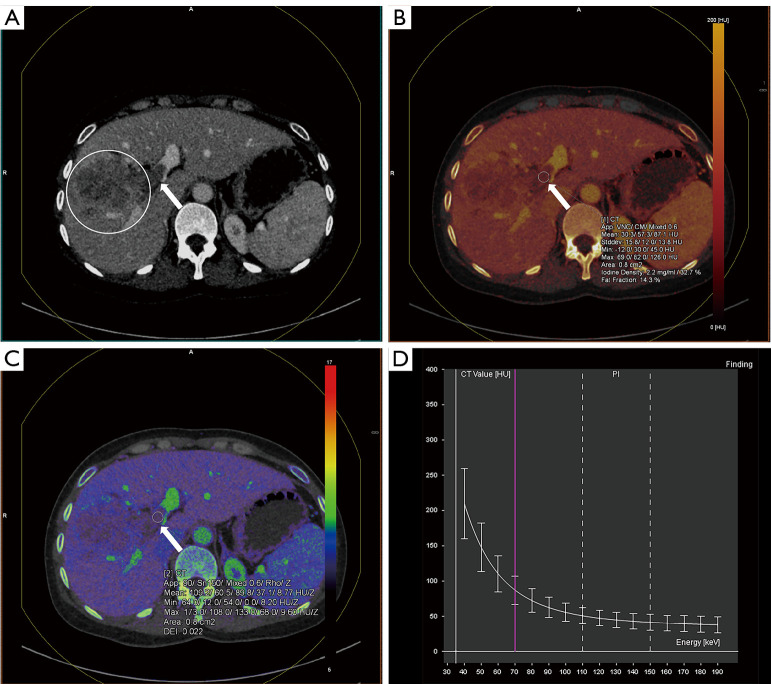
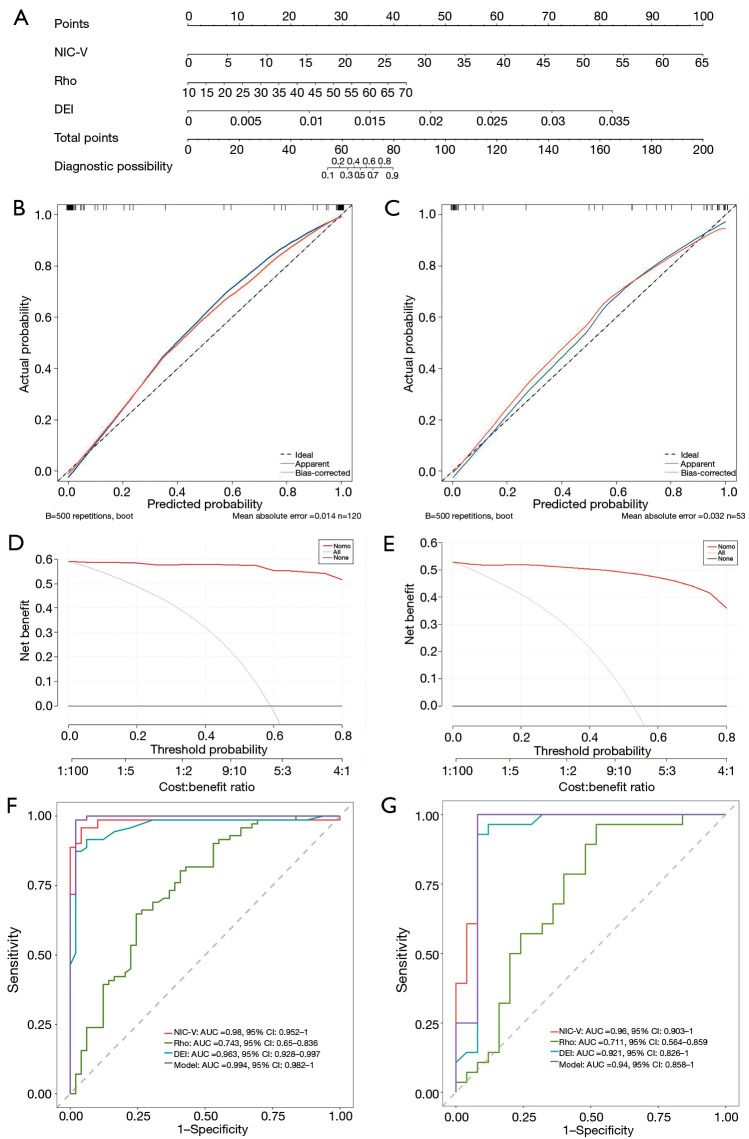
Methods: Computed tomography (CT) images of 173 patients with PVT (bland group, n=74; neoplastic group, n=99) were retrospectively analyzed. Portal venous phase iodine-based decomposition images were reconstructed to contrast iodine indices among groups, including thrombus iodine concentration (IC), normalized iodine concentration in the aorta (NIC-A), normalized iodine concentration in the portal vein (NIC-V), electron density (Rho), effective atomic number (Z), dual-energy index (DEI), and spectral slope (K). Diagnostic performance was evaluated using the area under the receiver operating characteristic curve (AUC), sensitivity, specificity, and accuracy. Univariate and multivariate analyses selected DECT parameters and created a nomogram for prediction.
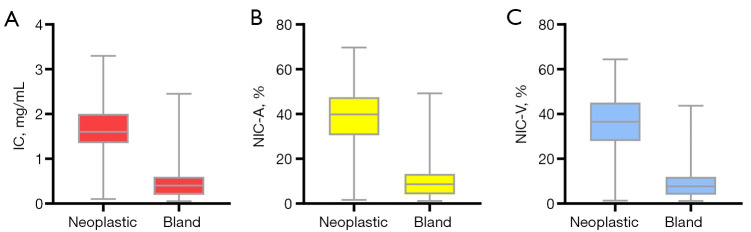
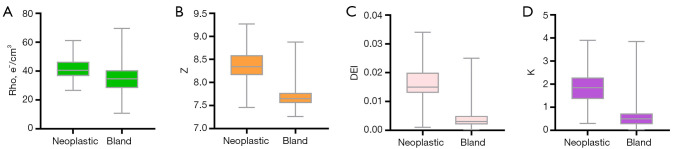
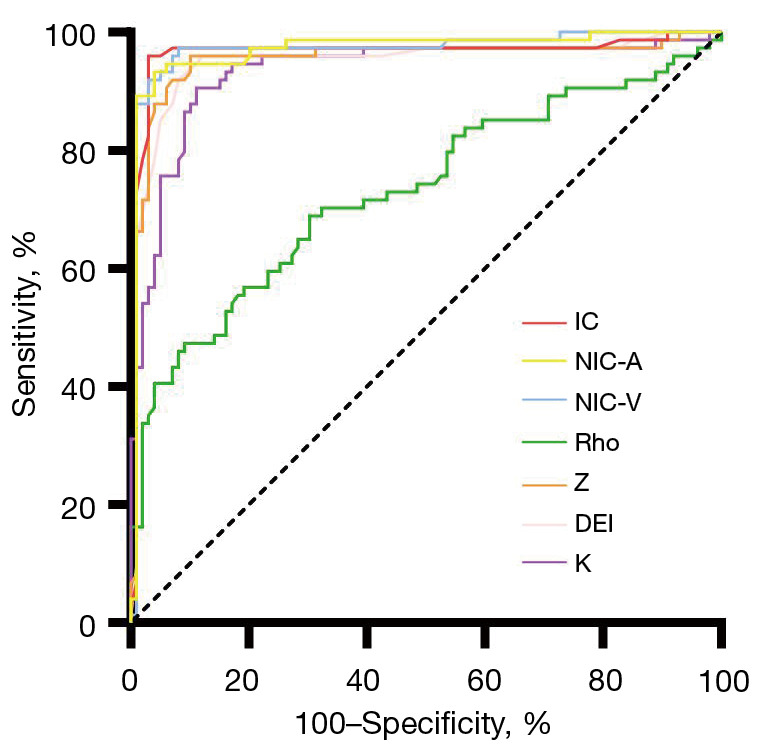
Results: (I) The values of IC, NIC-A, NIC-V, Rho, Z, DEI, and K were significantly higher in the neoplastic group compared to the bland group (P<0.001). (II) The AUC using IC, NIC-A, and NIC-V to differentiate between neoplastic and bland PVT were 0.963, 0.970, and 0.969, respectively; using Rho, Z, DEI, and K, they were 0.732, 0.952, 0.949, and 0.933, respectively. All the quantitative parameters achieved high sensitivity and high specificity in distinguishing neoplastic from bland PVT. (III) A nomogram was developed to predict neoplastic PVT probability; its AUC, sensitivity, and specificity reached remarkable levels, with values of 0.994, 98.59%, and 97.96% in the training cohort and 0.940, 100%, and 92.00% in the test cohort, respectively.
Conclusions: The DECT quantitative parameters demonstrate significant potential as non-invasive markers for distinguishing between neoplastic and bland PVT.
Keywords: Dual-energy computed tomography (DECT); dual-energy index (DEI); electron density; iodine concentration (IC); portal vein thrombosis (PVT).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2024-2516/coif). All authors report that this study was supported by the Science and Technology Program of Hunan Province (No. 2021SK50927). The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Dual-energy CT quantitative parameters for prediction of prognosis in patients with resectable rectal cancer.Eur Radiol. 2025 Aug;35(8):4945-4956. doi: 10.1007/s00330-025-11398-3. Epub 2025 Feb 8. Eur Radiol. 2025. PMID: 39921716
-
Feasibility of iodine concentration parameter and extracellular volume fraction derived from dual-energy CT for distinguishing type I and type II epithelial ovarian carcinoma.Abdom Radiol (NY). 2025 Jul;50(7):3238-3248. doi: 10.1007/s00261-024-04752-4. Epub 2024 Dec 12. Abdom Radiol (NY). 2025. PMID: 39665991
-
Dual-energy CT Radiomics Combined with Quantitative Parameters for Differentiating Lung Adenocarcinoma From Squamous Cell Carcinoma: A Dual-center Study.Acad Radiol. 2025 Mar;32(3):1675-1684. doi: 10.1016/j.acra.2024.09.024. Epub 2024 Sep 25. Acad Radiol. 2025. PMID: 39327138
-
Platelet count, spleen length, and platelet count-to-spleen length ratio for the diagnosis of oesophageal varices in people with chronic liver disease or portal vein thrombosis.Cochrane Database Syst Rev. 2017 Apr 26;4(4):CD008759. doi: 10.1002/14651858.CD008759.pub2. Cochrane Database Syst Rev. 2017. PMID: 28444987 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
LinkOut - more resources
Full Text Sources