

Validation of the Somnolyzer 24×7 automatic scoring system in children with suspected obstructive sleep apnea
- PMID: 40606446
- PMCID: PMC12213436
- DOI: 10.3389/fmed.2025.1617530
Validation of the Somnolyzer 24×7 automatic scoring system in children with suspected obstructive sleep apnea
Abstract
Introduction: Manual scoring of polysomnography data is a laborious and complex process. Automatic scoring by current computer algorithms shows high agreement with manual scoring. The primary objective of this study was to measure the overall validity of the Somnolyzer 24×7 automatic polysomnography scoring system in children.
Materials and methods: We conducted a single-center, prospective, observational study in children undergoing diagnostic polysomnography for suspected obstructive sleep apnea (OSA) from December 2023 to December 2024. We included children aged three to 15 years with suspected obstructive sleep apnea (OSA). Each polysomnogram was scored manually by three experts and automatically by the Somnolyzer 24×7 system.
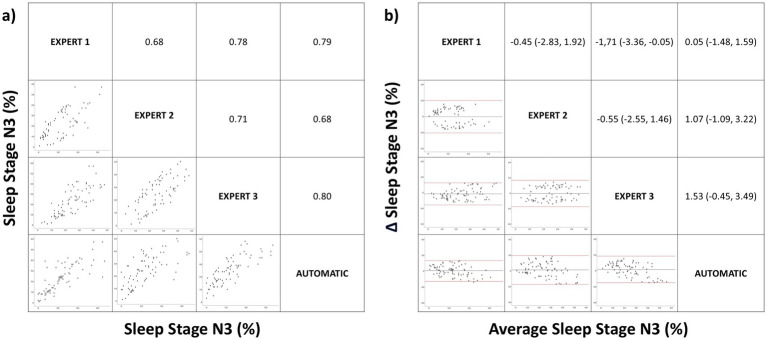
Results: Our analysis included 75 children (60% girls), of whom 9% did not have OSA, 20% had mild OSA, 31% moderate OSA, and 40% severe OSA. There was a high level of agreement between manual and automatic scoring of the respiratory disturbance index (RDI). The mean correlation (Pearson correlation coefficient) of RDI scored by the three experts was 0.93 (95% confidence interval [CI] 0.92-0.95), similar to the correlation between manual and automatic scoring (0.92, 95% CI 0.90-0.94). The correlation between the different manual scorings and between manual and automatic scoring was maintained in the different sleep stages (N1: 0.93 vs. 0.90, N2: 0.76 vs. 0.73, N3: 0.72 vs. 0.76, REM: 0.86 vs. 0.82).
Conclusion: The Somnolyzer 24×7 automatic scoring system shows strong correlation with manual scoring in respiratory events and sleep architecture. Our results suggest this system could be used for polysomnography scoring in children.
Keywords: Somnolyzer; artificial intelligence; children; obstructive sleep apnea; polysomnography; sleep disorders.
Copyright © 2025 Boira, Esteban, Sancho-Chust, Pastor, Fernández-Martínez, Torba and Chiner.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources