

Preliminary Radiographic Classification of First Metatarsal Osteotomy Healing Following Minimally Invasive Hallux Valgus Surgery
- PMID: 40606594
- PMCID: PMC12214334
- DOI: 10.1177/24730114251345818
Preliminary Radiographic Classification of First Metatarsal Osteotomy Healing Following Minimally Invasive Hallux Valgus Surgery
Abstract
Background: Minimally invasive or percutaneous surgery (MIS) for hallux valgus correction has seen increased adoption because of a growing evidence base of positive clinical and radiographic outcomes following surgery. However, no standardized or validated radiographic classification exists to evaluate the first metatarsal osteotomy healing following MIS hallux valgus surgery. The aim was to develop a new radiographic classification system for assessing bone healing following MIS distal transverse osteotomy for hallux valgus.
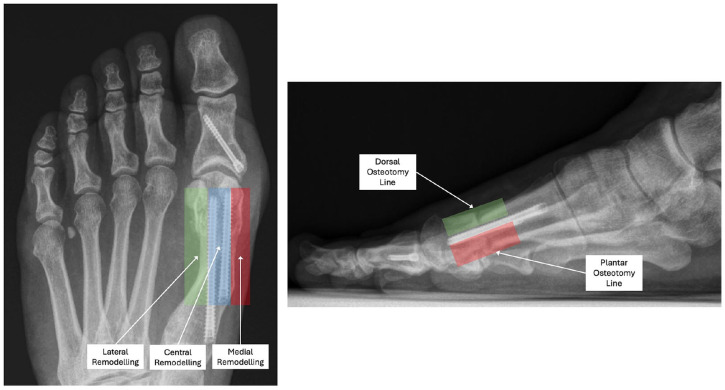
Methods: A 4-domain radiographic classification system based on callus formation, anteroposterior (AP) osteotomy line, lateral osteotomy line, and remodeling for MIS osteotomy healing was developed and tested on a cohort of 27 feet that underwent percutaneous transverse osteotomy for hallux valgus correction. Patients had simultaneous postoperative weightbearing computed tomography (WBCT) and standard radiographs following surgery. Five surgeons reviewed anonymized radiographs to evaluate interobserver reliability. WBCT was used to confirm union status and classification interpretation.
Results: The classification system demonstrated substantial interobserver reliability for lateral osteotomy line (Fleiss kappa = 0.671, 95% CI 0.505-0.814) and AP osteotomy line assessment (Fleiss kappa = 0.664, 95% CI 0.459-0.811), with moderate agreement for callus formation (κ = 0.465) and remodeling (κ = 0.439). The classification showed strong correlation with WBCT findings, with an optimal threshold of 8 points identified to differentiate union from nonunion, achieving an overall classification accuracy of 85.2%. This finding was supported by the area under the receiver operating characteristic (ROC) curve of 0.832. At the optimal threshold, the classification demonstrated 90.0% sensitivity and 71.4% specificity for detecting union.
Conclusion: This preliminary classification provides a reliable tool for assessing first metatarsal bone healing following MIS hallux valgus osteotomies, with substantial interobserver reliability. It offers a standardized approach for radiographic evaluation, which may enhance comparability across studies and serve as a radiographic research tool pending further validation. Its clinical applicability remains to be determined.
Level of evidence: Level III, diagnostic study.
Keywords: ROC curve; bone healing; classification system; hallux valgus; interobserver reliability; minimally invasive surgery; percutaneous osteotomy; radiographic assessment; reliability; weightbearing CT.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas L. Lewis, MBChB(Hons), BSc(Hons), FRCS(Tr&Orth), MFSTEd, reports royalties and consulting from Vilex beyond the scope of this study and PhD tuition fees supported by MIFAS. Jonathan Kaplan, MD, reports disclosures relevant to manuscript from royalties Enovis/DJO, staples; royalties from Treace Medical, hallux valgus implants; royalties from Vilex, calcaneal osteotomy; Artelon, paid consultancy; Edge Surgical, paid consultancy; and general disclosures from AOFAS Governance Committee Chair, unpaid; AOFAS Education Committee, unpaid; Foot & Ankle Orthopaedics journal editor, unpaid; Treace Medical, stock; GLW Medical Innovation, investor/stock options; Exactech (discontinued), surgeon advisory board; Surgical Fusion Inc (discontinued), consultant; and Royalty (soft tissue anchor). Tyler Gonzalez, MD, MBA, reports consultancy fees from Treace Medical Concepts Inc, Surgical Fusion Technologies, Stryker, Enovis, Exactech, and Surgebright and royalties from Surgical Fusion Technologies, Treace Medical Concepts, and Vilex, all outside scope of this study. Robbie Ray, MBChB, ChM(T&O), FRCSEd(Tr&Orth), FEBOT, reports prospective royalty payments from Enovis/Novastep and payment for honoraria, lectures, presentations, and speakers fees from Enovis/Novastep, Medartis/IBRA, and Marquardt UK, beyond the scope of this study. Peter Lam, MBBS(Hons), FRACS, reports royalties from Enovis, consulting fees from Enovis and Paragon 28, and payment from AOFAS for Kenneth Johnson Lecture 2024. All fees outside the scope of this manuscript. Disclosure forms for all authors are available online.
Figures






References
-
- Audigé L, Bhandari M, Hanson B, Kellam J. A concept for the validation of fracture classifications. J Orthop Trauma. 2005;19(6):401-406. - PubMed
-
- Blitz NM, Wong DT, Grecea B, Baskin ES. Characterization of first metatarsal regeneration after new modern minimally invasive bunion surgery. A retrospective radiographic review of 172 cases. J Minim Invasive Bunion Surg. 2024;1:92756. doi: 10.62485/001c.92756 - DOI
LinkOut - more resources
Full Text Sources
Research Materials