

Human albumin infusion for reducing hyponatremia and circulatory dysfunction in liver cirrhosis: A meta-analysis update
- PMID: 40606931
- PMCID: PMC12210167
- DOI: 10.4254/wjh.v17.i6.106418
Human albumin infusion for reducing hyponatremia and circulatory dysfunction in liver cirrhosis: A meta-analysis update
Abstract
Background: Liver cirrhosis is a progressive disease with high morbidity and mortality requiring effective management strategies to improve patient outcomes. Various therapies including albumin infusion, volume expanders (VEs), and vasoactive agents are used to manage patients with cirrhosis. Despite numerous clinical trials, a comprehensive meta-analysis comparing the effectiveness of albumin infusion against alternative treatments is limited. This study provides the current and comprehensive synthesis of evidence, offering key insights for optimizing therapeutic strategies in patients with liver cirrhosis.
Aim: To systematically update available data on therapies of liver cirrhosis, we performed a meta-analysis to evaluate and compare the clinical efficacy of albumin infusion vs other VEs and vasoactive agents in patients with liver cirrhosis.
Methods: A literature search from the PubMed and Embase databases (inception till June 2024) focused on hyponatremia (primary outcome) and various outcomes such as gastrointestinal bleeding, hepatic encephalopathy, severe infection, post-paracentesis-induced circulatory dysfunction (PICD), ascites reappearance, spontaneous bacterial peritonitis, hepatorenal syndrome, renal impairment, hospital stay, mortality, and safety was performed. The primary analysis pooled studies that compared albumin infusion with control. In the subgroup analysis, comparisons were made within the stratified treatment categories included in the control group.
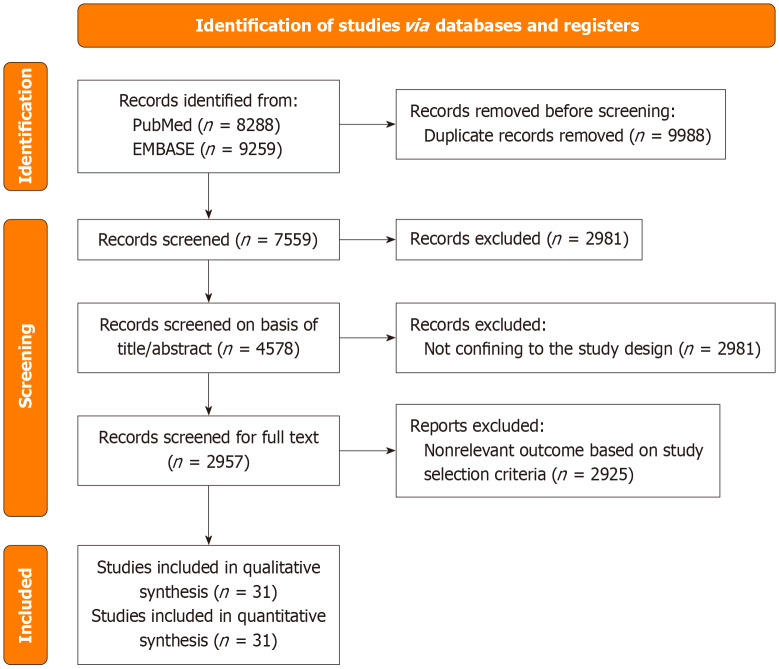
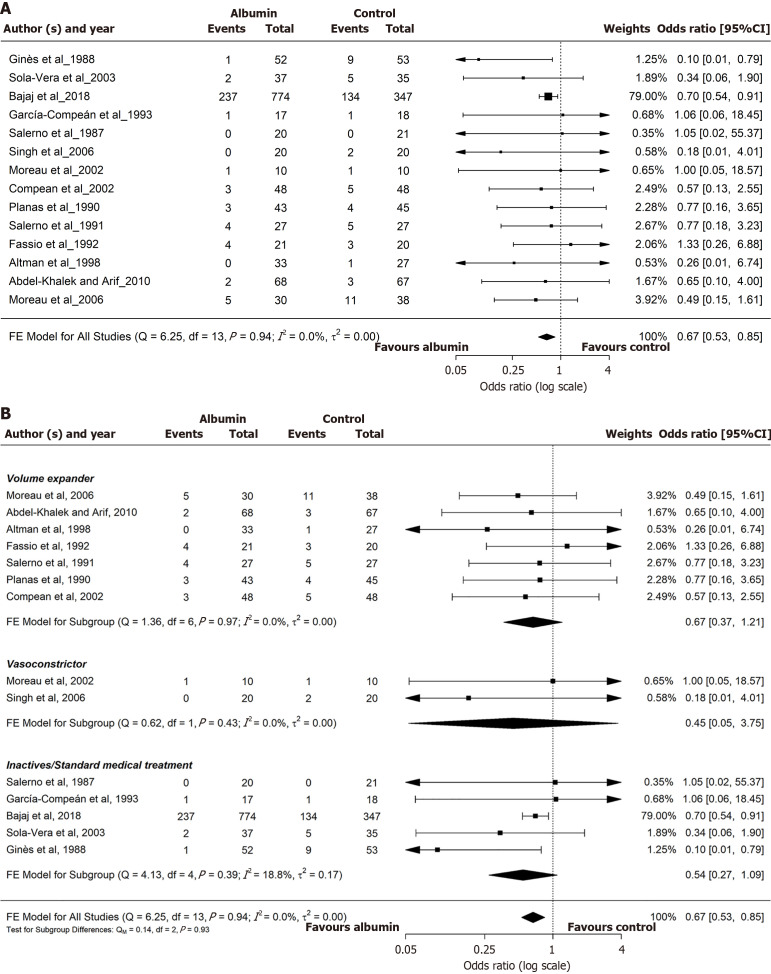
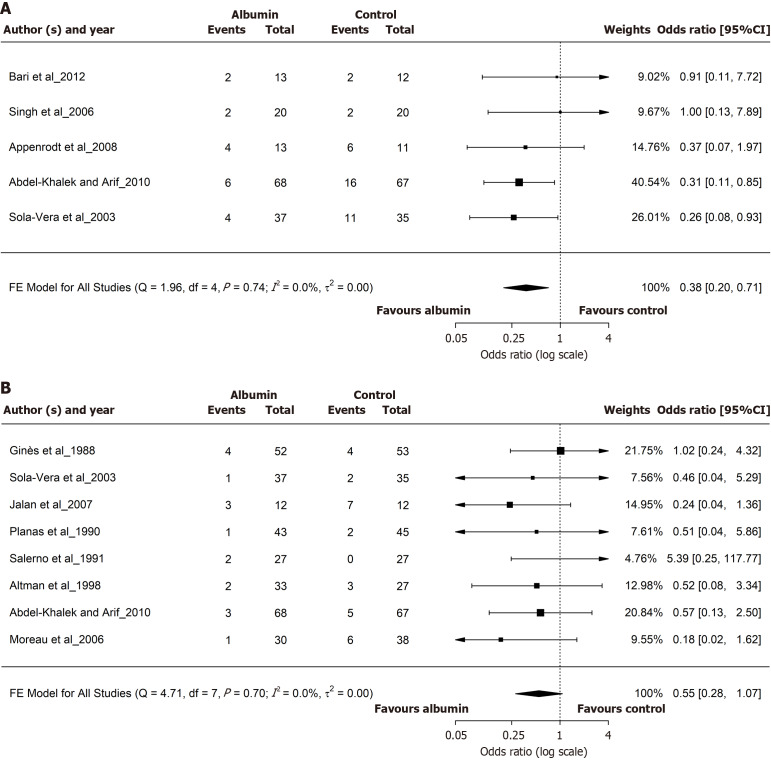
Results: Of the 2957 studies retrieved, 31 studies (27 randomized controlled trials and 4 observational studies) comprising 6255 patients were included. Albumin use was significant in reducing odds of hyponatremia [odds ratio (OR) = 0.67; 95% confidence interval (95%CI) = 0.53-0.85] and PICD (OR = 0.38; 95%CI = 0.20-0.71), whereas the reduction in severe infection (OR = 0.55; 95%CI = 0.28-1.07) did not reach statistical significance. In the subgroup analysis, albumin demonstrated a favorable improvement in lowering the incidence of hyponatremia vs inactive/standard medical therapy (OR = 0.54; 95%CI = 0.27-1.09). For PICD, albumin use was significant compared with other VEs (OR = 0.31; 95%CI = 0.11-0.85) but not with vasoconstrictors (OR = 0.63; 95%CI = 0.21-1.91). In the overall subgroup analysis, a significant reduction was observed in hyponatremia (OR = 0.67; 95%CI = 0.53-0.85) and PICD (OR = 0.38; 95%CI = 0.20-0.71).
Conclusion: Human albumin has been shown to significantly reduce the incidence of hyponatremia and PICD in patients with liver cirrhosis, whereas its effect on severe infection remains suggestive but not statistically significant.
Keywords: Albumin; Efficacy; Hepatic encephalopathy; Hyponatremia; Liver cirrhosis; Mortality; Paracentesis-induced circulatory dysfunction; Safety.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors have no conflicts of interest to declare.
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Volume expanders for the prevention of ovarian hyperstimulation syndrome.Cochrane Database Syst Rev. 2016 Aug 31;2016(8):CD001302. doi: 10.1002/14651858.CD001302.pub3. Cochrane Database Syst Rev. 2016. PMID: 27577848 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Nutritional support for liver disease.Cochrane Database Syst Rev. 2012 May 16;2012(5):CD008344. doi: 10.1002/14651858.CD008344.pub2. Cochrane Database Syst Rev. 2012. PMID: 22592729 Free PMC article.
References
LinkOut - more resources
Full Text Sources
