

Airway management by ambulance nurses during out-of-hospital cardiac arrest
- PMID: 40607043
- PMCID: PMC12214125
- DOI: 10.1016/j.resplu.2025.100999
Airway management by ambulance nurses during out-of-hospital cardiac arrest
Abstract
Background: Adequate airway management in out-of-hospital cardiac arrest (OHCA) is crucial for ventilation and oxygenation. Advanced airway management with a supraglottic airway device (SAD) or endotracheal tube (ETT) follows bag-valve-mask (BVM) ventilation, with emergency front-of-neck access as a rescue-option. EMS protocols on airway management in OHCA have changed over the years and during the COVID-pandemic. This study assessed subsequent changes in airway management and the success of different strategies.
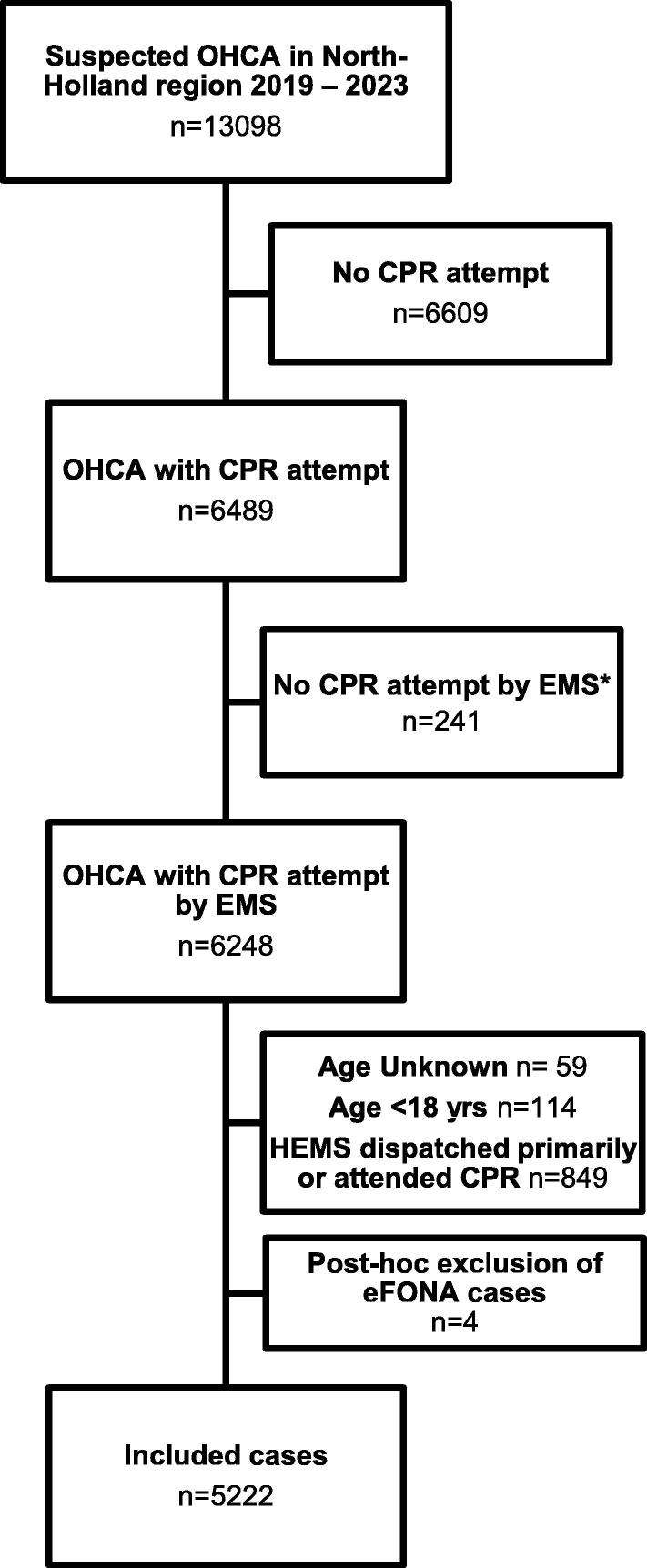
Methods: An observational study was conducted with data from ARREST, 2019-2023. All consecutive adult OHCA patients who had resuscitation attempted by EMS were included. Patients were excluded if helicopter emergency medical services were involved. Changes in devices used intra-arrest and their first-pass success were analyzed.
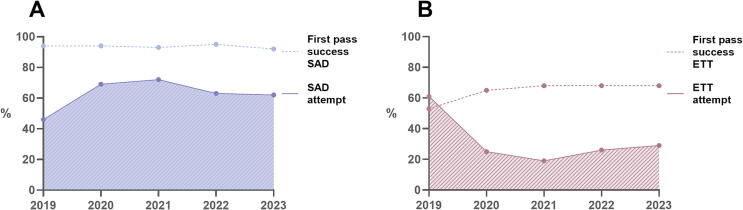
Results: The proportion of cases with an SAD attempt increased, and with an ETT decreased. The definitive airway device used was an SAD in 59% (95% CI: 57-60%), an ETT in 21% (95% CI: 19-22%), and BVM in 14% (95% CI: 13-15%). First pass success for ETT increased from 53% to 68%. Average SAD first pass success was 93%.
Conclusion: During cardiopulmonary resuscitation (CPR) by ambulance nurses, the use of SADs increased, and that of ETTs decreased. Although ETT first pass success improved, it was lower than the guideline-recommended standard for performing intubations prehospitally. First pass success for SAD was high. This adds support for current Dutch ambulance guidelines recommending an SAD for primary choice of advanced airway by EMS during CPR. However, improvement of intubation techniques and skills remain a necessity for selected OHCA patients.
Keywords: Advanced Life Support (ALS); Airway management; Cardiac Arrest; Cardiopulmonary Resuscitation (CPR); Emergency Medical Services (EMS); Ventilation.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: ‘LD and HvS report a grant to their institution from Stryker Emergency Care. JdJ and VE report no conflict of interest. PS reports a grant from Health Holland, outside the scope of this study. MWH reports grants to his institution from ZonMW and ESAIC, and consulting fees paid to his institution from IDD Pharma, Medical Developments and PAION, all outside the scope of this study.’.
Figures

References
-
- Lurie K.G., Nemergut E.C., Yannopoulos D., Sweeney M. The physiology of cardiopulmonary resuscitation. Anesth Analg. 2016;122:767–783. - PubMed
-
- van Schuppen H., Boomars R., Kooij F.O., den Tex P., Koster R.W., Hollmann M.W. Optimizing airway management and ventilation during prehospital advanced life support in out-of-hospital cardiac arrest: a narrative review. Best Pract Res Clin Anaesthesiol. 2021;35:67–82. - PubMed
-
- Wang C.H., Lee A.F., Chang W.T., et al. Comparing effectiveness of initial airway interventions for out-of-hospital cardiac arrest: a systematic review and network meta-analysis of clinical controlled trials. Ann Emerg Med. 2020;75:627–636. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
