

Association between metabolic-associated fatty liver disease and risk of cardiometabolic multimorbidity: a disease trajectory analysis in UK Biobank
- PMID: 40607218
- PMCID: PMC12213339
- DOI: 10.3389/fendo.2025.1585725
Association between metabolic-associated fatty liver disease and risk of cardiometabolic multimorbidity: a disease trajectory analysis in UK Biobank
Abstract
Objective: While metabolic-associated fatty liver disease (MAFLD) has been associated with individual cardiometabolic diseases (CMDs), its role in the dynamic progression to cardiometabolic multimorbidity (CMM) remains unclear. We investigated the association of MAFLD, its severity and subtypes with CMM in individuals with no or one CMD at baseline.
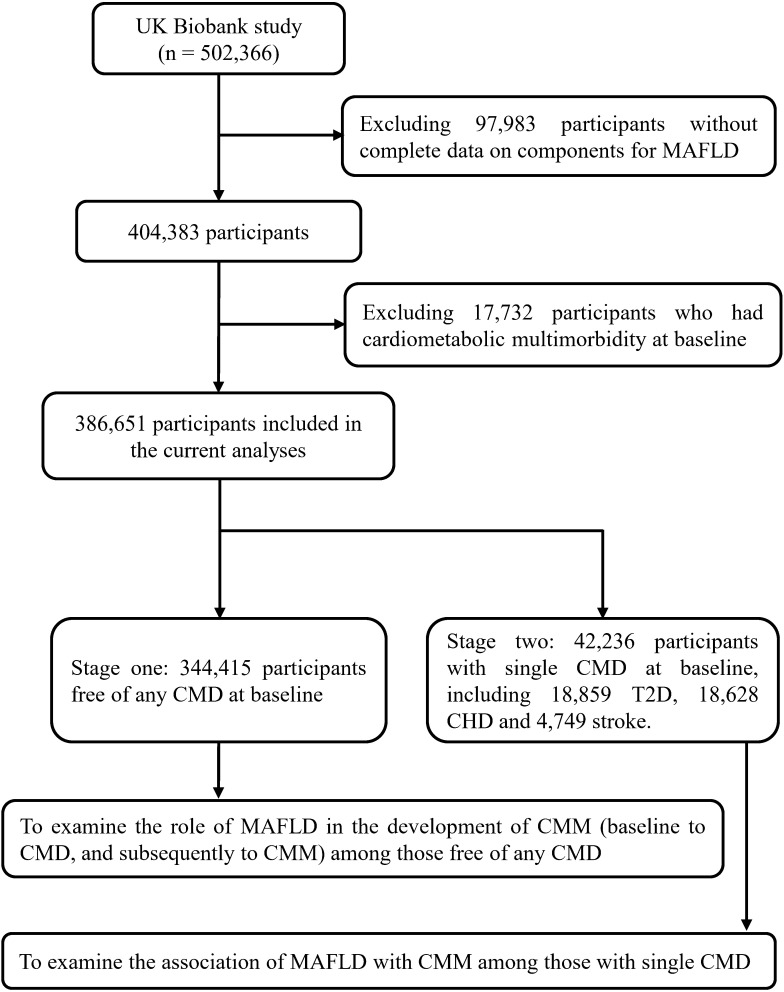
Methods: This prospective cohort study involved 386,651 individuals (344,415 without and 42,236 with a single CMD at baseline) from the UK Biobank. MAFLD was defined as the presence of hepatic steatosis plus overweight/obesity, type 2 diabetes (T2D), or metabolic abnormalities. CMM was defined as the coexistence of two or more CMDs in the same person, including T2D, coronary heart disease (CHD) and stroke. Cox proportional hazard models and multistate models were performed to estimate the hazard ratios (HRs) and 95% confidence intervals (95% CIs).
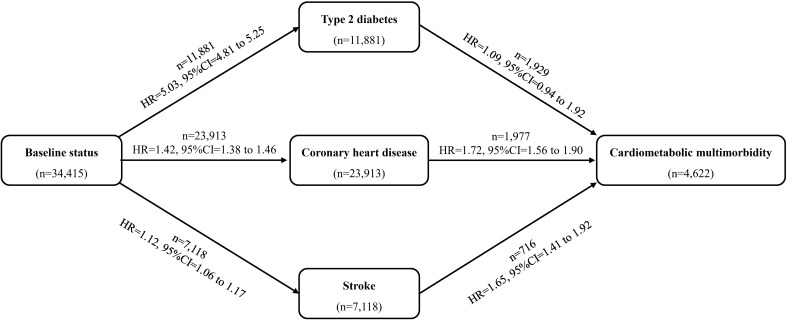
Results: During a median follow-up of 13.85 years, 4,622 new-onset CMM cases emerged among participants free of CMD at baseline. MAFLD was significantly associated with an increased risk of incident CMM (adjusted HR: 2.78, 95% CI: 2.60-2.96). Multistate models showed that MAFLD adversely affected most transitions from baseline to single CMDs and then to CMM. Among the single-CMD participants, the adjusted HRs of incident CMM in the MAFLD group were 1.21 (95% CI: 1.13-1.31) for T2D patients, 1.90 (1.75-2.05) for CHD patients, and 1.65 (1.45-1.87) for stroke patients, respectively.
Conclusion: MAFLD independently elevated the risk of incident CMM, regardless of the baseline CMD status. These findings emphasize the necessity of targeted MAFLD interventions for CMM prevention.
Keywords: UK Biobank; cardiometabolic multimorbidity; disease trajectory; metabolic-associated fatty liver disease; multistate model.
Copyright © 2025 Gao, Yao, Liu, Yin, Jia, Huang, Zhao and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Kuan V, Denaxas S, Patalay P, Nitsch D, Mathur R, Gonzalez-Izquierdo A, et al. Identifying and visualising multimorbidity and comorbidity patterns in patients in the English National Health Service: a population-based study. Lancet Digital Health. (2023) 5:e16–27. doi: 10.1016/s2589-7500(22)00187-x - DOI - PubMed
-
- Zhao Y, Atun R, Oldenburg B, McPake B, Tang S, Mercer SW, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Global Health. (2020) 8:e840–9. doi: 10.1016/s2214-109x(20)30127-3 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical