

Sex-specific differences in the relationship between the atherogenic index and hypertension in middle-aged and elderly Chinese
- PMID: 40607234
- PMCID: PMC12213374
- DOI: 10.3389/fendo.2025.1574125
Sex-specific differences in the relationship between the atherogenic index and hypertension in middle-aged and elderly Chinese
Abstract
Background: Despite the already comprehensive epidemiological evidence concerning pre-hypertension, high-normal blood pressure, and hypertension, the influence of gender differences within this context remains inadequately explored. The present study endeavors to meticulously examine the specific impact of the plasma atherogenic index (AIP) on pre-hypertension and hypertension, and ascertain whether there exist significant sex-specific differences in this regard.
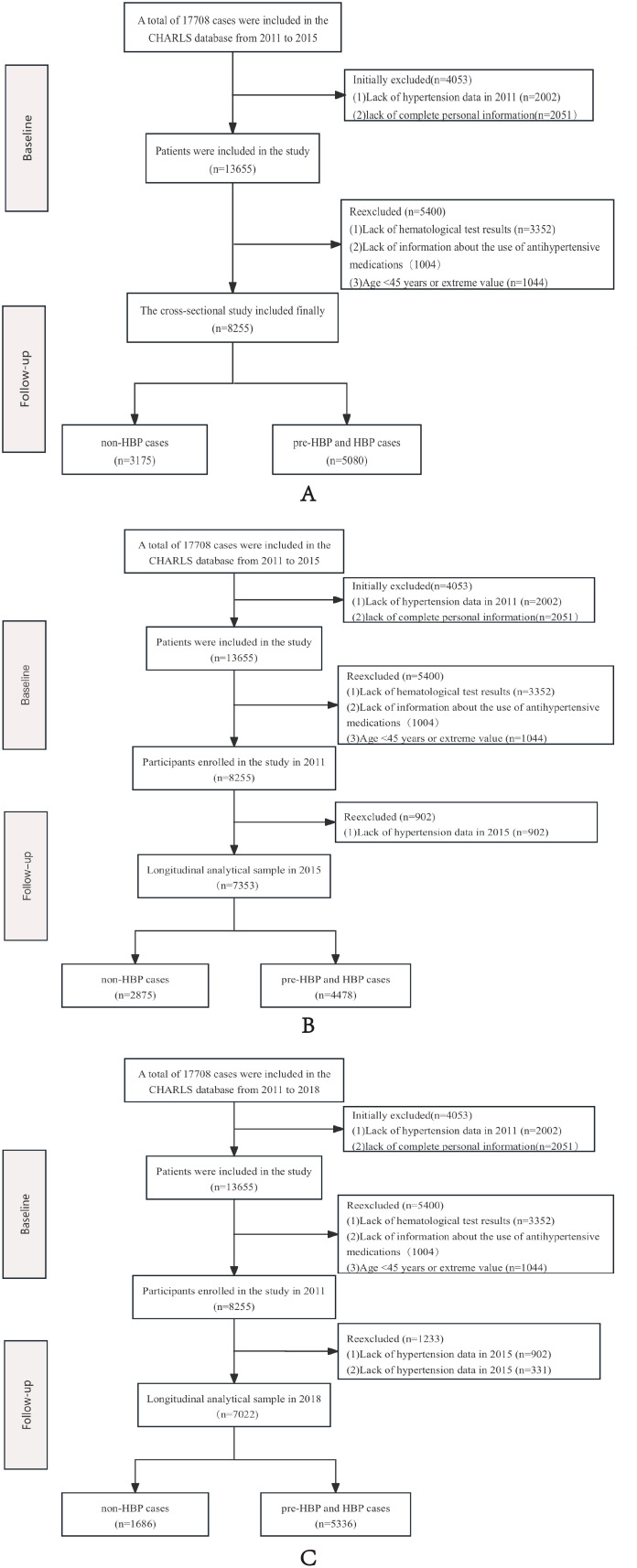
Methods: This population-based study employed a multi-wave cohort design encompassing 8255 middle-aged and elderly participants (cross-sectional phase) and longitudinal follow-ups in 2015 (n=8092) and 2018 (n=7022). Participants were stratified into normotensive (n=3175 in cross-sectional, n=2415 in 2015 longitudinal cohort study, 1868 in 2018 longitudinal cohort study) and prehypertensive/hypertensive groups (n=5080 (61.5%) in cross-sectional study, n=5677(70.2%) in longitudinal study of 2015, n=5336(76.0%) in 2018). The plasma atherogenic index=log10(triglycerides/high-density lipoprotein)[triglycerides (mg/dL)/HDL-C (mg/dL)]) was quantified enzymatically. Multivariable-adjusted logistic regression models with restricted cubic splines were implemented to evaluate nonlinear associations between AIP and blood pressure status, adjusting for age, sex, BMI, smoking, and lipid-lowering therapy. Sensitivity analyses included multiple imputation for missing covariates and sex-stratified effect modification testing.
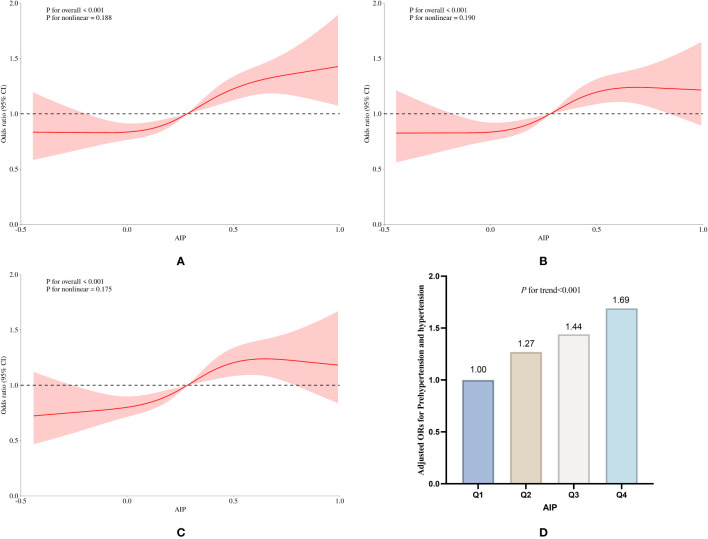
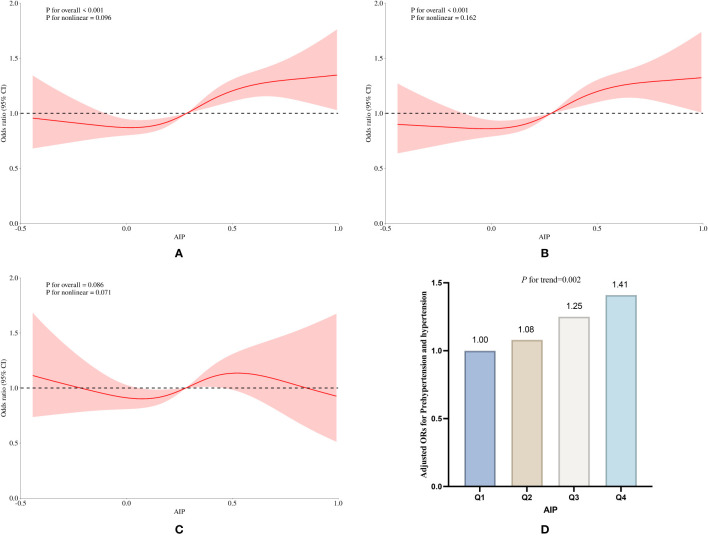
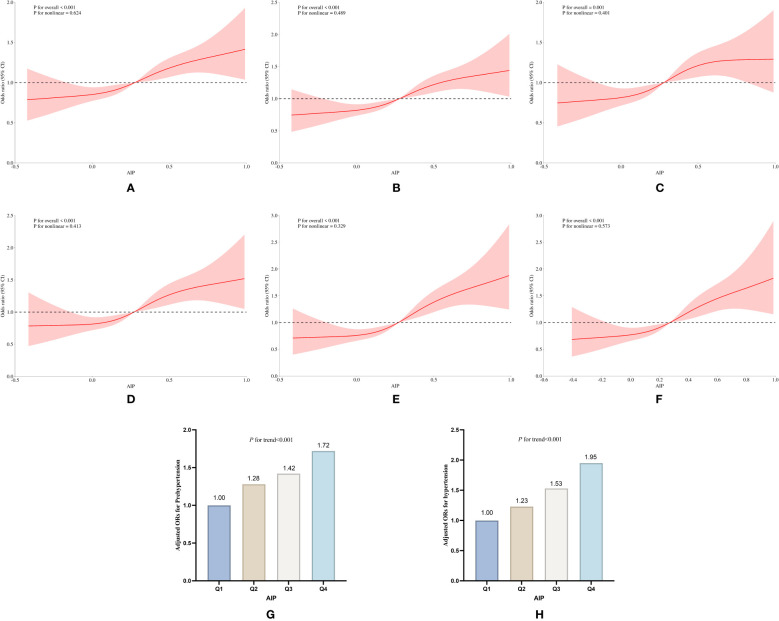
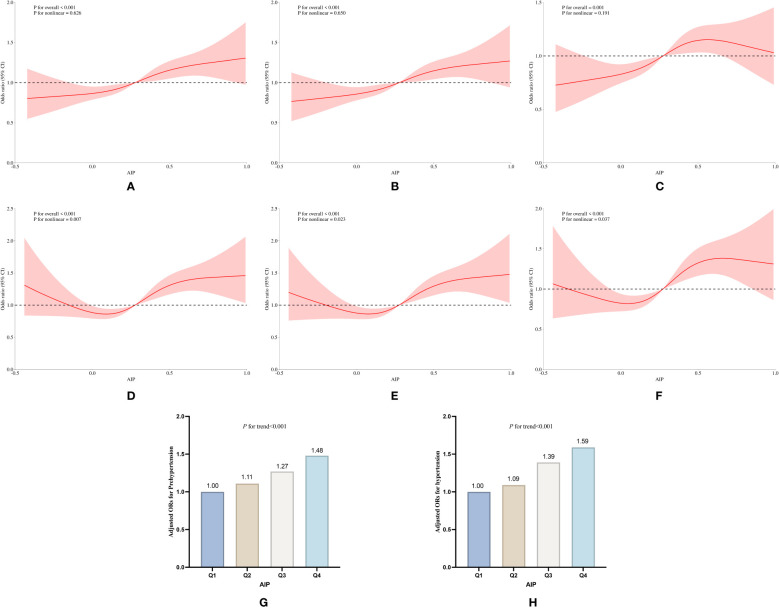
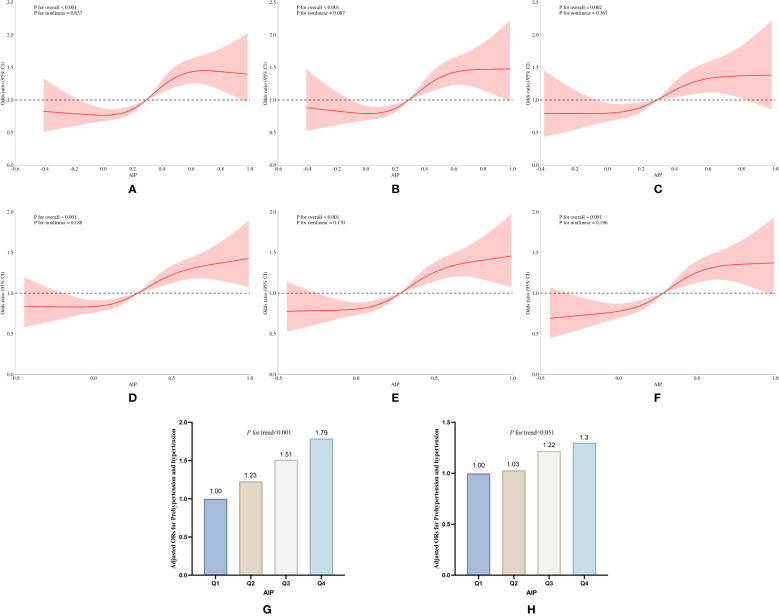
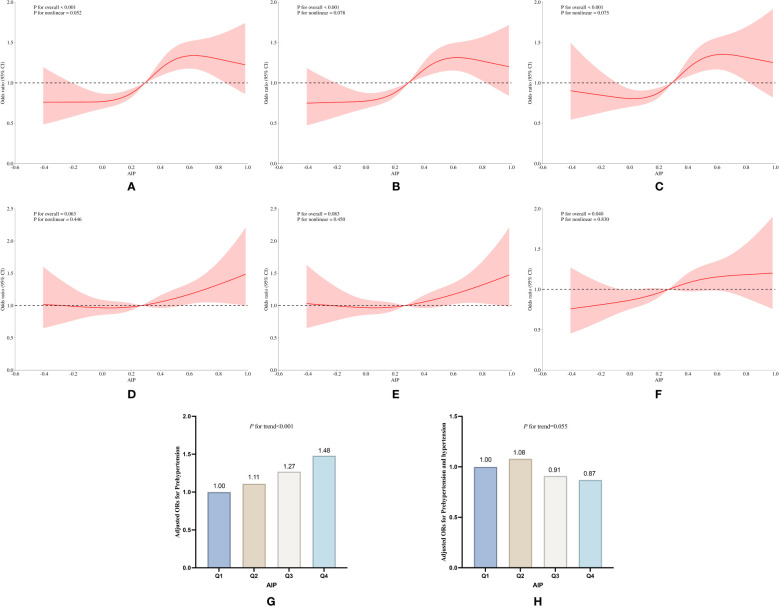
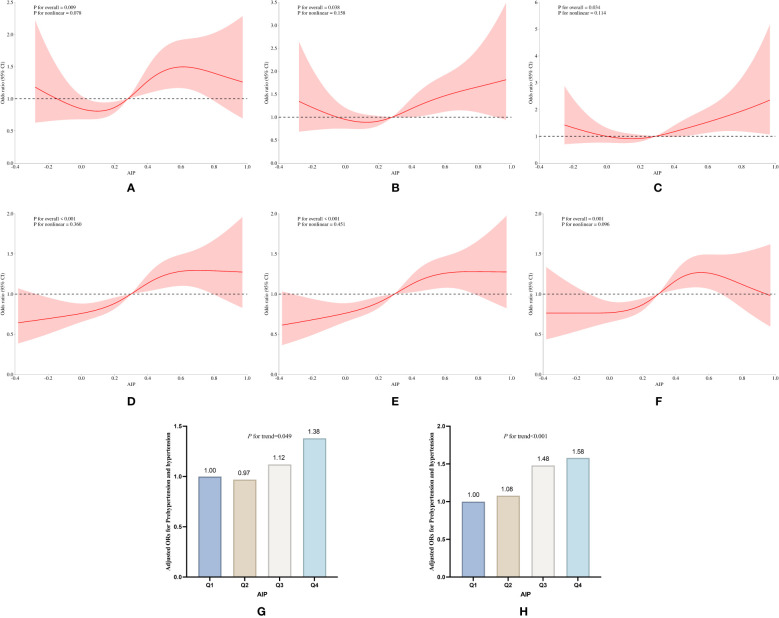
Results: This epidemiological investigation revealed population prevalences of 34.3% for pre-hypertension and 27.2% for hypertension. Both cross-sectional and longitudinal analyses demonstrated a significant positive association between AIP index and blood pressure dysregulation. Adjusted logistic regression models showed that elevated AIP corresponded to increased risks of pre-hypertension/hypertension, with cross-sectional analyses yielding an odds ratio (OR) of 1.69 (95% CI:1.38 to 2.07, P<0.001). Longitudinal cohorts of 2015 and 2018 exhibited persistent temporal trends: OR=1.38 (95% CI:1.13 to 1.67, P=0.012) in 2015 and OR=1.41 (95% CI:1.20 to 1.65, P<0.001) in 2018. Sex-stratified analyses revealed markedly stronger associations in females, where each AIP unit increase conferred a 1.79-fold cross-sectional risk elevation (OR: 1.79, 95% CI:1.35 to 2.38, P < 0.001), rising to 1.49-fold (2015 cohort: OR: 1.49, 95% CI: 1.14 to 1.95, P=0.003) and 1.64-fold (2018 cohort: OR: 1.64, 95% CI:1.31 to 2.06, P<0.001) in longitudinal assessments. Conversely, males exhibited attenuated associations (cross-sectional OR: 1.30; 95% CI:1.12 to 1.79, P=0.006; 2015 longitudinal OR: 1.26, 95% CI:1.12 to 1.66), with nonsignificant effects in the 2018 follow-up (OR: 0.87, 95% CI:0.57 to 1.31). A significant gender-AIP interaction (P<0.001) underscored sex-specific metabolic susceptibility to atherogenic lipid profiles.
Conclusion: This study identified a significant positive association between elevated atherogenic index of plasma levels and blood pressure dysregulation. Both cross-sectional and longitudinal analyses consistently demonstrated a dose-response relationship, with higher AIP levels associated with increased risk. Stratified analyses by sex revealed that the association between elevated AIP and the incidence of pre-hypertension and hypertension was significantly stronger in women.
Keywords: atherogenic index of plasma; female; hypertension; pre-hypertension; sex-specific differences.
Copyright © 2025 Zhang, Wang, Kong, Li, Bao, Tu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association of Atherogenic Index of Plasma With Stroke Risk in a Population With Cardiovascular-Kidney-Metabolic Syndrome Stages 0 to 3: The First Evidence From the China Health and Retirement Longitudinal Study.J Am Heart Assoc. 2025 Jul 15;14(14):e039983. doi: 10.1161/JAHA.124.039983. Epub 2025 Jul 14. J Am Heart Assoc. 2025. PMID: 40654258
-
Relationship between plasma atherogenic index and incidence of cardiovascular diseases in Chinese middle-aged and elderly people.Sci Rep. 2025 Mar 13;15(1):8775. doi: 10.1038/s41598-025-86213-6. Sci Rep. 2025. PMID: 40082452 Free PMC article.
-
Association between atherogenic index of plasma and hypertension combined with diabetes mellitus in United States adults: an analysis of the NHANES surveys from 2011 to 2016.J Health Popul Nutr. 2025 Jul 30;44(1):269. doi: 10.1186/s41043-025-01013-y. J Health Popul Nutr. 2025. PMID: 40739270 Free PMC article.
-
Effect of cocoa on blood pressure.Cochrane Database Syst Rev. 2017 Apr 25;4(4):CD008893. doi: 10.1002/14651858.CD008893.pub3. Cochrane Database Syst Rev. 2017. PMID: 28439881 Free PMC article.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous