

Effectiveness and safety of different electromagnetic stimulation therapies in treating post-stroke insomnia: A network meta-analysis of randomized controlled trials
- PMID: 40608764
- PMCID: PMC12225873
- DOI: 10.1371/journal.pone.0327544
Effectiveness and safety of different electromagnetic stimulation therapies in treating post-stroke insomnia: A network meta-analysis of randomized controlled trials
Abstract
Objectives: To evaluate the efficacy and safety of different electromagnetic therapies for the treatment of post-stroke insomnia (PSI). Thus, we conducted a network meta-analysis to provide evidence-based insights for clinical practice.
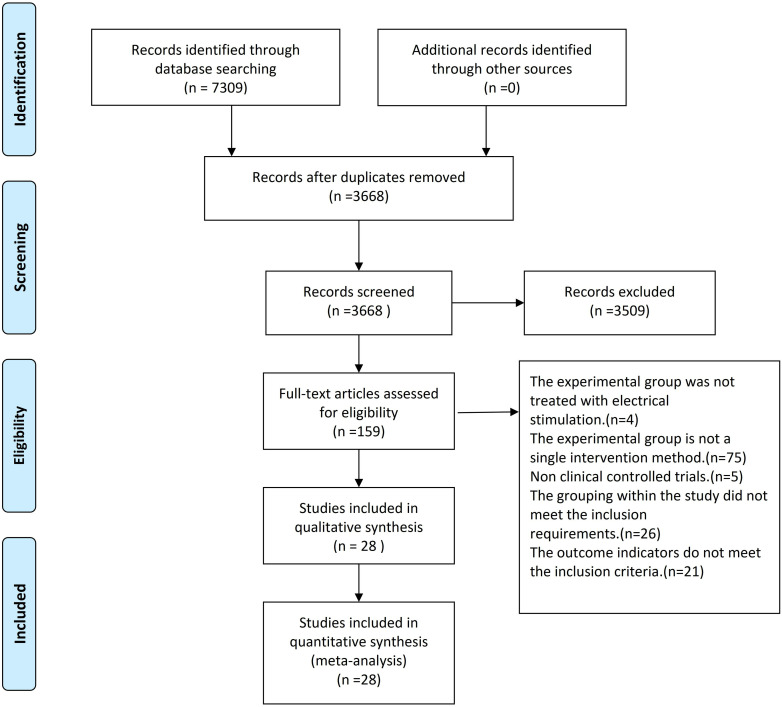
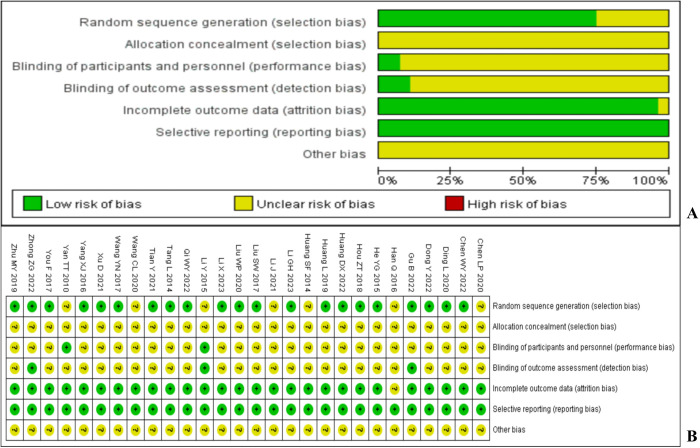
Methods: Databases such as PubMed, Excerpt Medica Database (Embase), Cochrane Library Central Register of Controlled Trials, APA PsycInfo, China National Knowledge Infrastructure Database, Wanfang, and SinoMed were used to retrieve randomized controlled trials (RCTs) on electromagnetic therapy for PSI, with a search deadline of Sep 2024 for each database. The Cochrane bias risk assessment tool was used to evaluate the quality of the included RCTs. Stata was used for network meta-analysis.
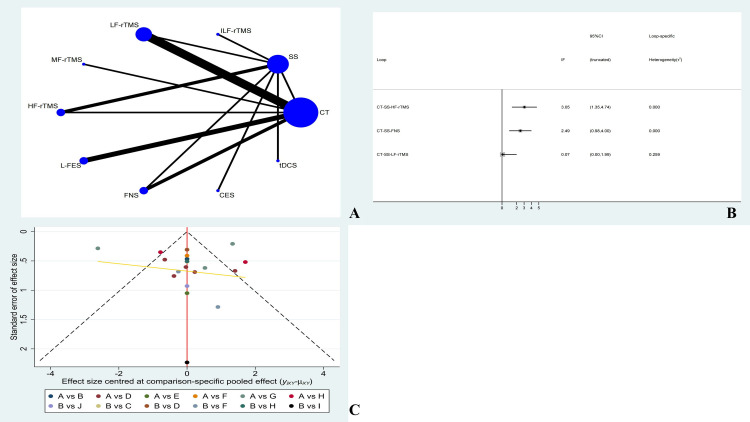
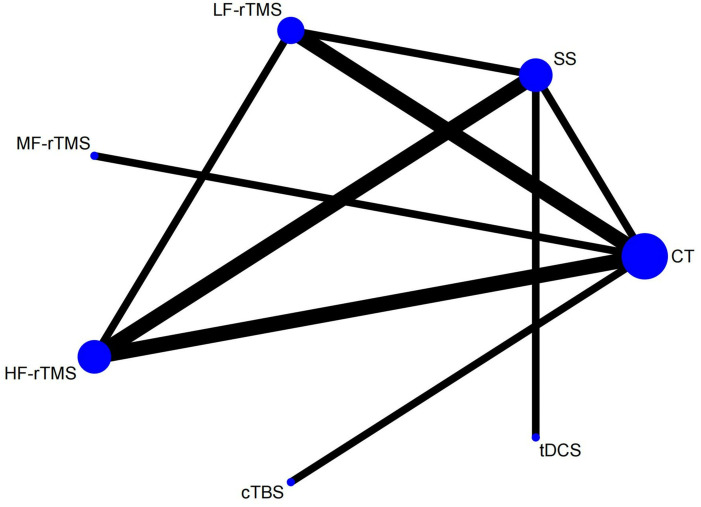
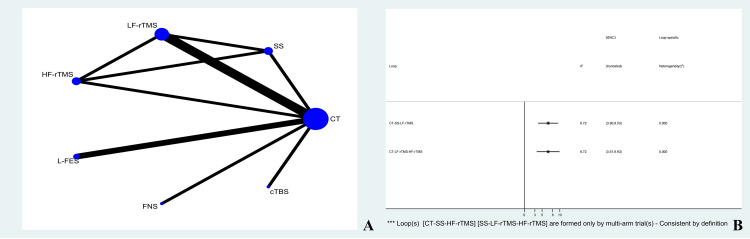
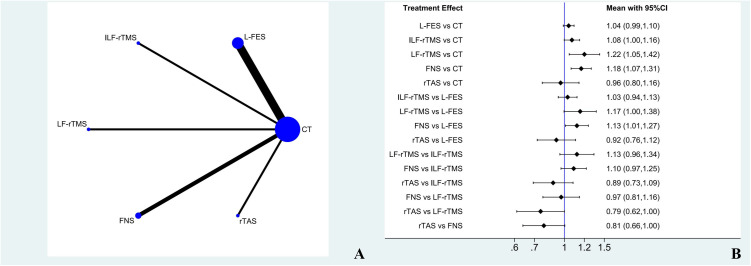
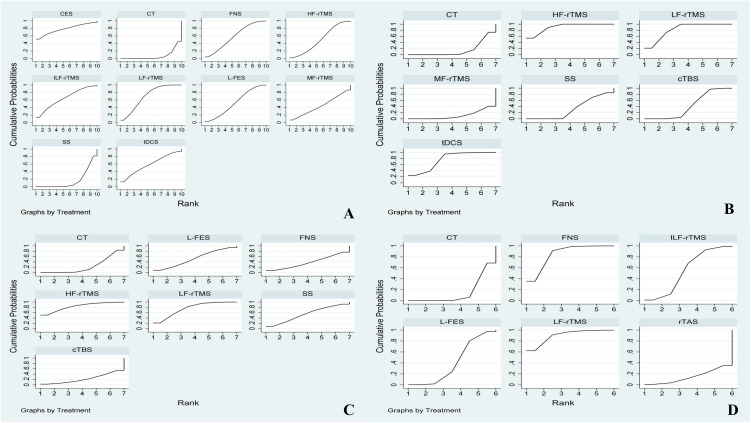
Results: We included 28 RCTs involving 2353 patients across 12 different treatment regimens. The surface under the cumulative ranking results showed that the ranking of Pittsburgh sleep quality index decline was: cranial electrotherapy stimulation>low frequency repetitive transcranial magnetic stimulation (LF-rTMS)>infra-low frequency repetitive transcranial magnetic stimulation (ILF-rTMS)>fastigial nucleus stimulation (FNS)>transcranial direct current stimulation (tDCS)>low frequency electric stimulation (L-FES)>high frequency repetitive transcranial magnetic stimulation (HF-rTMS)>middle frequency repetitive transcranial magnetic stimulation (MF-rTMS)>sham stimulation (SS)>common treatment (CT); Ranking of Hamilton depression scale decline degree: HF-rTMS > LF-rTMS > tDCS > SS>continuous theta-burst stimulation (cTBS)>MF-rTMS > CT; national Institute of health stroke scale decline ranking: HF-rTMS > LF-rTMS > SS > L-FES>electroencephalographic biomimetic stimulation>CT > cTBS; Clinical total effective rate ranking: LF-rTMS > FNS > ILF-rTMS > L-FES > CT>repetitive transcranial acupuncture stimulation.
Conclusions: Different electromagnetic therapies can effectively improve sleep quality in PSI patients, and the efficacy and safety of LF-rTMS are significant. However, owing to the limitations of this study, the efficacy ranking cannot fully explain the advantages and disadvantages of clinical efficacy. In the future, additional multicentre, large-sample, double-blind, clinical, and randomized controlled trials are required to supplement and demonstrate the results of this study.
Strengths and limitations of this study: This is the first study to conduct network meta-analysis on PSI treatment with different electromagnetic therapies. Simultaneously, we refined the classification based on different frequency patterns of the same therapy, and the results can serve as a reference for clinical workers. This study had some limitations: A large proportion of low-quality literature may lead to biased results; Lack of subgroup analysis, mainly because the number of studies included was not very high, and the quality of most studies was low. Basic information such as stroke site and onset time were not detailed, which may increase the possibility of inconsistency and clinical heterogeneity. After all, detailed subgroup analysis based on the stage or location of stroke can provide more meaningful clinical guidance.
Copyright: © 2025 Sun et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
