

Development and validation of a BMI stratified mortality prediction model for patients with COPD complicated by HF using the MIMIC-IV database
- PMID: 40610557
- PMCID: PMC12229611
- DOI: 10.1038/s41598-025-09605-8
Development and validation of a BMI stratified mortality prediction model for patients with COPD complicated by HF using the MIMIC-IV database
Abstract
Given the high mortality rate of chronic obstructive pulmonary disease (COPD) complicated by heart failure (HF), early identification of high-risk patients and timely intervention are crucial. There is currently no in-hospital mortality risk prediction model for COPD complicated by HF patients with different Body Mass Index (BMI). This study aims to explore the risk factors of COPD complicated by HF and construct an in-hospital mortality risk prediction model.
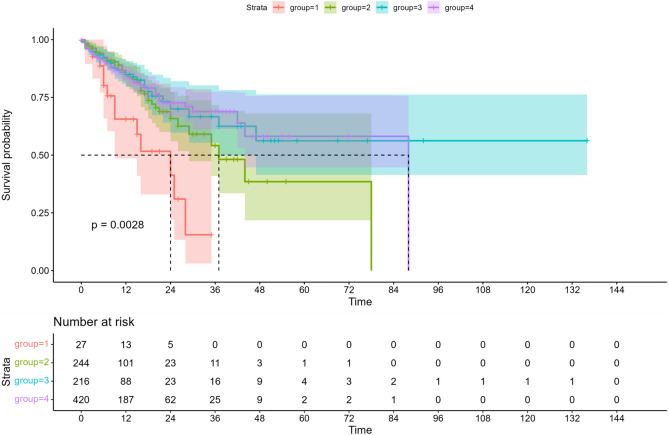
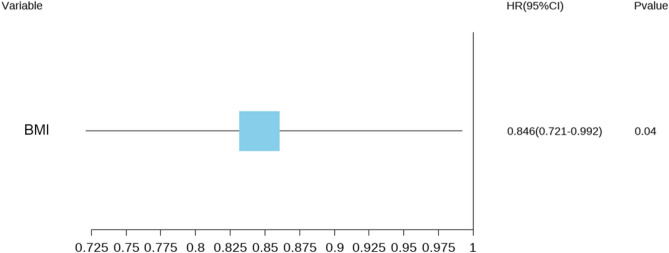
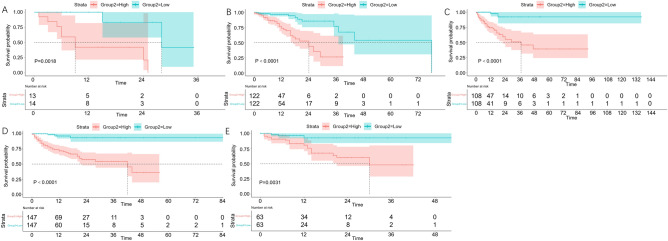
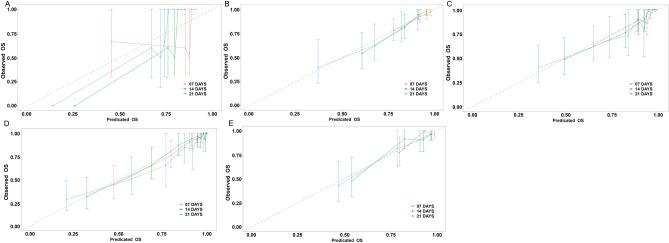
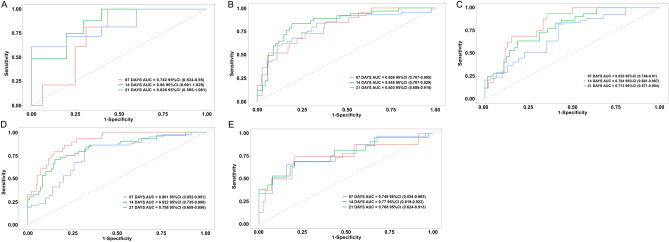
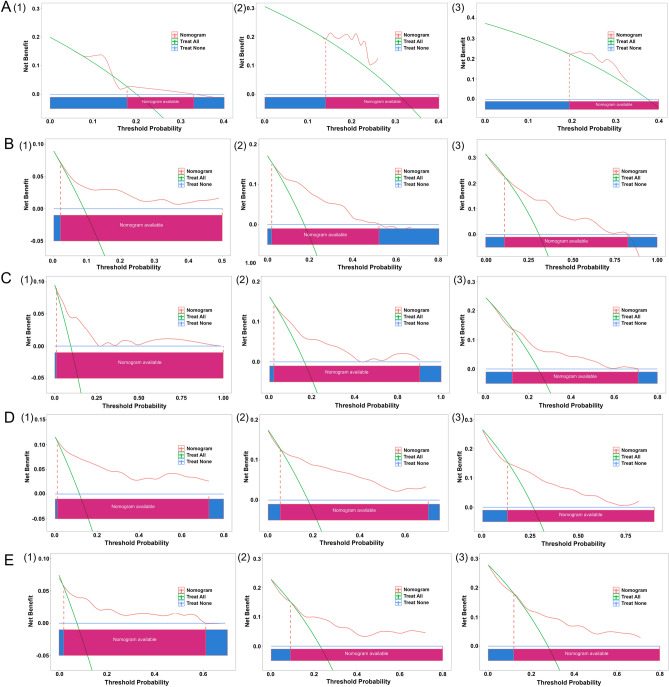
Method: Select a population that meets the diagnostic criteria for COPD complicated by HF from the Medical Information Mart for Intensive Care IV (MIMIC-IV) and analyze the baseline characteristics of the patients. Univariate Cox regression analysis and multivariate Cox regression analysis were used to determine the risk factors for mortality in patients with different BMIs and to construct a prediction model. Evaluate the model's consistency, discriminability, and clinical application value using the calibration curve, area under the curve (AUC), and decision curve analysis (DCA), respectively.
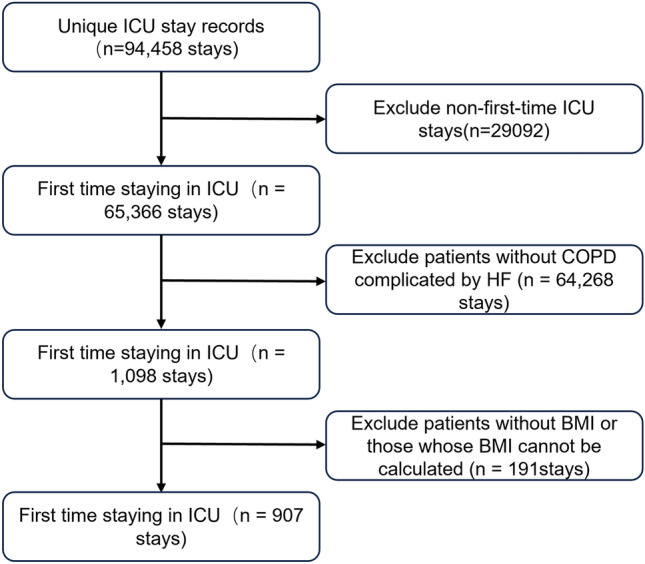
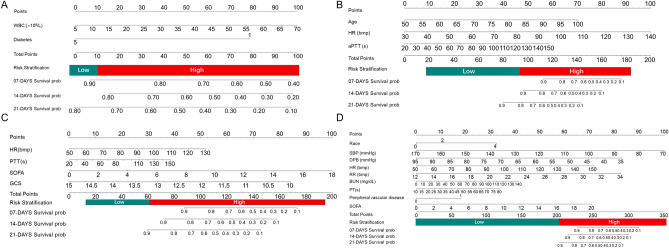
Result: A total of 907 patients with COPD complicated by HF were included, and risk factors such as age, heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), white blood cell count (WBC), heart rate(HR), respiratory rate (RR), blood urea nitrogen (BUN), prothrombin time (PT), activated partial thromboplastin time (aPTT), diabetes, peripheral vascular disease, sequential organ failure assessment (SOFA), and Glasgow Coma Scale(GCS) were included in the prediction model. AUC, calibration, and decision curves indicate that most models have good discrimination, calibration, and clinical application value.
Conclusion: The in-hospital mortality risk prediction model for COPD complicated by HF based on MIMIC-IV has good recognition ability and significant clinical reference value for patient prognosis risk assessment and intervention treatment.
Keywords: Body Mass Index; Chronic obstructive pulmonary disease; Heart failure; In-hospital mortality prediction model; MIMIC database.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Construction and validation of a nomogram prediction model for death risk in patients with chronic obstructive pulmonary disease complicated by hypercapnic respiratory failure in the intensive care unit.Respir Med. 2025 Aug-Sep;245:108188. doi: 10.1016/j.rmed.2025.108188. Epub 2025 Jun 1. Respir Med. 2025. PMID: 40460897
-
Are Current Survival Prediction Tools Useful When Treating Subsequent Skeletal-related Events From Bone Metastases?Clin Orthop Relat Res. 2024 Sep 1;482(9):1710-1721. doi: 10.1097/CORR.0000000000003030. Epub 2024 Mar 22. Clin Orthop Relat Res. 2024. PMID: 38517402
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.Health Technol Assess. 2001;5(26):1-149. doi: 10.3310/hta5260. Health Technol Assess. 2001. PMID: 11701099
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
References
-
- Shi, Q., Xu, J., Zeng, L., Lu, Z. & Chen, Y. A nomogram for predicting short-term mortality in ICU patients with coexisting chronic obstructive pulmonary disease and congestive heart failure. Respir Med.10.1016/j.rmed.2024.107803 (2024). - PubMed
-
- Horwich, T. B., Fonarow, G. C. & Clark, A. L. Obesity and the Obesity Paradox in Heart Failure. Prog. Cardiovasc Dis.61, 151–156. 10.1016/j.pcad.2018.05.005 (2018). - PubMed
-
- Jieyun, Z. et al. Body mass index and mortality of chronic obstructive pulmonary disease: a meta-analysis. Chin. J. Evid. Based Med.19, 811–817 (2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
