

Role of electrograms recorded from mini electrodes in catheter ablation of atrioventricular nodal reentrant tachycardia: a retrospective study
- PMID: 40610905
- PMCID: PMC12226832
- DOI: 10.1186/s12872-025-04924-0
Role of electrograms recorded from mini electrodes in catheter ablation of atrioventricular nodal reentrant tachycardia: a retrospective study
Abstract
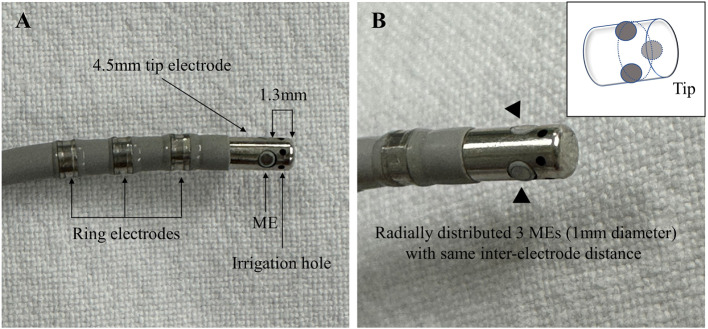
Background: Data on the role of electrograms (EGMs) recorded from mini electrodes (MEs) of the IntellaTip MiFi ablation catheter (Boston Scientific) are limited. We evaluated the additional value of MEs during slow-pathway ablation in atrioventricular nodal reentrant tachycardia (AVNRT).
Methods: Consecutive patients with AVNRT who underwent slow-pathway ablation using the MiFi catheter were included. A combined electroanatomical approach was used to identify the target site. During ablation, operators were blinded to the ME EGMs, and ME EGMs recorded immediately before the first radiofrequency (RF) application were evaluated retrospectively.
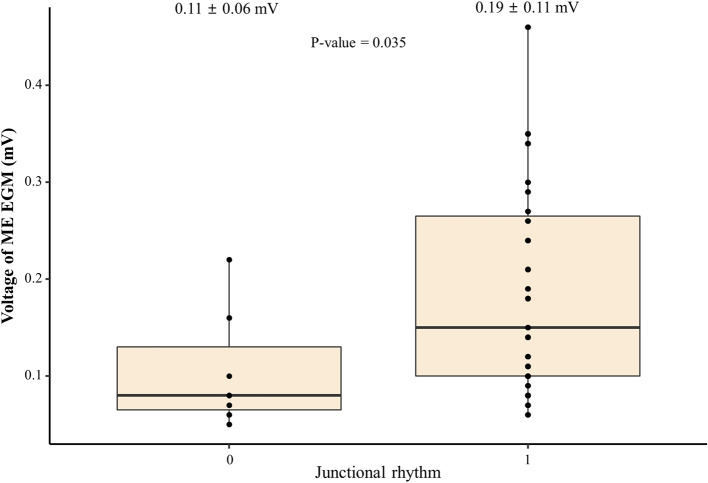
Results: Altogether, 61 patients with typical (n = 58), atypical (n = 2), or both (n = 1) of AVNRT were included. Successful slow-pathway ablation or modification was achieved in all patients, and 33 patients (54.1%) demonstrated a junctional rhythm during the first RF application. Atrial EGMs (> 0.05 mV) at the MEs were observed immediately before the first RF in 34 patients (55.7%). A significant association was identified between the presence of atrial EGMs in MEs and the occurrence of junctional rhythm (odds ratio 13.5, P < 0.001). The positive and negative predictive values of atrial EGMs in the MEs for junctional rhythm induction during the first RF were 79.4% (27/34) and 77.8% (21/27), respectively.
Conclusions: Atrial EGMs recorded from MEs before the first RF application could help identify effective ablation sites during slow-pathway ablation. Junctional rhythm was more frequently induced at sites with discernible ME signals, whereas sites without measurable ME EGMs despite adequate bipolar signals were less effective. These findings are limited to the initial RF application and warrant further validation.
Keywords: Atrioventricular nodal reentrant tachycardia; Catheter ablation; Mini electrodes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was reviewed and approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (approval number: 2024 − 0790; approval date: 19 Jun 2024), which waived the requirement for informed consent due to the retrospective nature of the study. All methods were performed in accordance with the relevant guidelines and regulations, including the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Unexpected transient atrioventricular block and slow junctional rhythm using pulsed field ablation for slow pathway modification: Excited or cautious for ablators.Heart Rhythm. 2025 Jul;22(7):1682-1692. doi: 10.1016/j.hrthm.2024.09.023. Epub 2024 Sep 19. Heart Rhythm. 2025. PMID: 39304002
-
Cryoablation versus radiofrequency ablation of atrioventricular nodal reentrant tachycardia.J Interv Card Electrophysiol. 2014 Mar;39(2):111-9. doi: 10.1007/s10840-013-9842-2. Epub 2013 Nov 29. J Interv Card Electrophysiol. 2014. PMID: 24293174
-
Efficacy and safety between radiofrequency ablation and types of cryoablation catheters for atrioventricular nodal reentrant tachycardia: A Network Meta-analysis and Systematic Review.Pacing Clin Electrophysiol. 2024 Mar;47(3):353-364. doi: 10.1111/pace.14915. Epub 2024 Jan 11. Pacing Clin Electrophysiol. 2024. PMID: 38212906
-
Comparative utility of omnipolar and bipolar electroanatomic mapping methods to detect and localize dual nodal substrate in patients with atrioventricular nodal reentrant tachycardia.J Interv Card Electrophysiol. 2024 Oct;67(7):1579-1591. doi: 10.1007/s10840-024-01800-3. Epub 2024 Apr 18. J Interv Card Electrophysiol. 2024. PMID: 38634991 Free PMC article.
-
Paradigm Shift for Catheter Ablation of Atypical Atrioventricular Nodal Re-Entrant Tachycardia: 3-Dimensional Mapping-Based Ablation.JACC Clin Electrophysiol. 2023 Aug;9(8 Pt 3):1730-1740. doi: 10.1016/j.jacep.2023.04.028. Epub 2023 Jun 21. JACC Clin Electrophysiol. 2023. PMID: 37354187
References
-
- Haissaguerre M, Gaita F, Fischer B, Commenges D, Montserrat P, d’Ivernois C, Lemetayer P, Warin JF. Elimination of atrioventricular nodal reentrant tachycardia using discrete slow potentials to guide application of radiofrequency energy. Circulation. 1992;85(6):2162–75. - PubMed
-
- Jackman WM, Beckman KJ, McClelland JH, Wang X, Friday KJ, Roman CA, Moulton KP, Twidale N, Hazlitt HA, Prior MI, et al. Treatment of supraventricular tachycardia due to atrioventricular nodal reentry by radiofrequency catheter ablation of slow-pathway conduction. N Engl J Med. 1992;327(5):313–8. - PubMed
-
- Feldman A, Voskoboinik A, Kumar S, Spence S, Morton JB, Kistler PM, Sparks PB, Vohra JK, Kalman JM. Predictors of acute and long-term success of slow pathway ablation for atrioventricular nodal reentrant tachycardia: a single center series of 1,419 consecutive patients. Pacing Clin Electrophysiol. 2011;34(8):927–33. - PubMed
-
- Chrispin J, Misra S, Marine JE, Rickard J, Barth A, Kolandaivelu A, Ashikaga H, Tandri H, Spragg DD, Crosson J, et al. Current management and clinical outcomes for catheter ablation of atrioventricular nodal re-entrant tachycardia. Europace. 2018;20(4):e51–9. - PubMed
-
- Jentzer JH, Goyal R, Williamson BD, Man KC, Niebauer M, Daoud E, Strickberger SA, Hummel JD, Morady F. Analysis of junctional ectopy during radiofrequency ablation of the slow pathway in patients with atrioventricular nodal reentrant tachycardia. Circulation. 1994;90(6):2820–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
