

Endoscopic Recanalization of a Long Segment Esophageal Obstruction Using the Combined Antegrade and Retrograde Rendezvous Procedure
- PMID: 40612797
- PMCID: PMC12225991
- DOI: 10.14309/crj.0000000000001754
Endoscopic Recanalization of a Long Segment Esophageal Obstruction Using the Combined Antegrade and Retrograde Rendezvous Procedure
Abstract
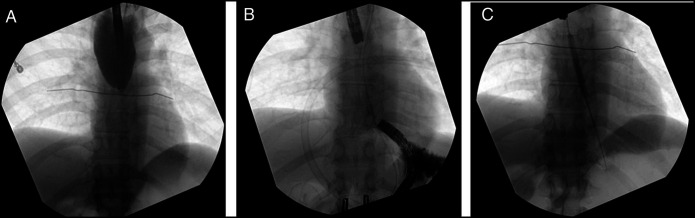
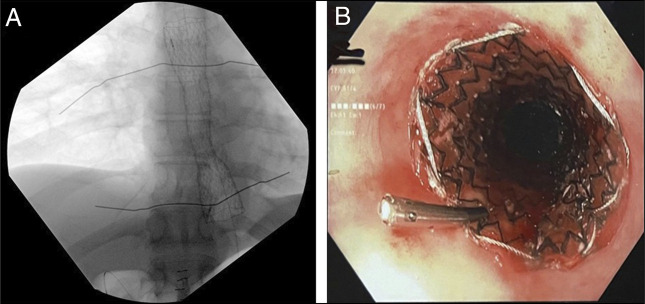
The combined antegrade and retrograde endoscopic rendezvous technique effectively restores patency for esophageal short-segment obstructing strictures (<3 cm). However, long-segment strictures typically require complex surgery, with endoscopic management rarely reported. We report a 44-year-old man with a 9 cm esophageal obstruction due to peptic stricture who was at high risk of esophageal resection due to severe cardiac disease and prior abdominal surgeries. He underwent successful recanalization using a rendezvous technique. Serial dilations with subsequent esophageal stenting restored luminal patency. This case highlights the feasibility of an endoscopic approach as a safe and effective alternative to surgery in long-segment peptic strictures.
Keywords: endoscopic dilation; esophageal stricture; rendezvous technique; stricture management.
© 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Figures

Similar articles
-
Endoscopic and surgical treatment of refractory caustic esophageal strictures.Surg Endosc. 2025 Jul;39(7):4513-4524. doi: 10.1007/s00464-025-11820-3. Epub 2025 May 30. Surg Endosc. 2025. PMID: 40447898
-
Laparoscopic-endoscopic rendezvous versus preoperative endoscopic sphincterotomy in people undergoing laparoscopic cholecystectomy for stones in the gallbladder and bile duct.Cochrane Database Syst Rev. 2018 Apr 11;4(4):CD010507. doi: 10.1002/14651858.CD010507.pub2. Cochrane Database Syst Rev. 2018. PMID: 29641848 Free PMC article.
-
When banding goes bad: two rare complications of endoscopic variceal banding ligation.Proc (Bayl Univ Med Cent). 2025 Jan 24;38(4):558-560. doi: 10.1080/08998280.2025.2452126. eCollection 2025. Proc (Bayl Univ Med Cent). 2025. PMID: 40557200 Free PMC article.
-
The allium stent for the complex ureteral stricture-deeper experience of a series case review.BJUI Compass. 2025 Jul 1;6(7):e70042. doi: 10.1002/bco2.70042. eCollection 2025 Jul. BJUI Compass. 2025. PMID: 40599592 Free PMC article.
-
Oncologic and Safety Outcomes for Retrograde and Antegrade Endoscopic Surgeries for Upper Tract Urothelial Carcinoma: A Systematic Review and Meta-analysis.Eur Urol Focus. 2023 Mar;9(2):258-263. doi: 10.1016/j.euf.2022.11.014. Epub 2022 Nov 22. Eur Urol Focus. 2023. PMID: 36428210
References
-
- Barkley C, Orringer MB, Iannettoni MD, Yee J. Challenges in reversing esophageal discontinuity operations. Ann Thorac Surg. 2003;76(4):989–95. - PubMed
-
- Ruigómez A, Alberto García Rodríguez L, Wallander M-A, Johansson S, Eklund S. Esophageal stricture: Incidence, treatment patterns, and recurrence rate. Am J Gastroenterol. 2006;101(12):2685–92. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
