

Safety and immunogenicity of investigational tuberculosis vaccine M72/AS01E-4 in people living with HIV in South Africa: an observer-blinded, randomised, controlled, phase 2 trial
- PMID: 40614747
- PMCID: PMC12310912
- DOI: 10.1016/S2352-3018(25)00124-9
Safety and immunogenicity of investigational tuberculosis vaccine M72/AS01E-4 in people living with HIV in South Africa: an observer-blinded, randomised, controlled, phase 2 trial
Abstract
Background: M72/AS01E-4 is a recombinant fusion protein vaccine candidate derived from two Mycobacterium tuberculosis antigens (Mtb32A and Mtb39A) and AS01E-4 adjuvant. We evaluated safety and immunogenicity of M72/AS01E-4 in people living with HIV in South Africa.
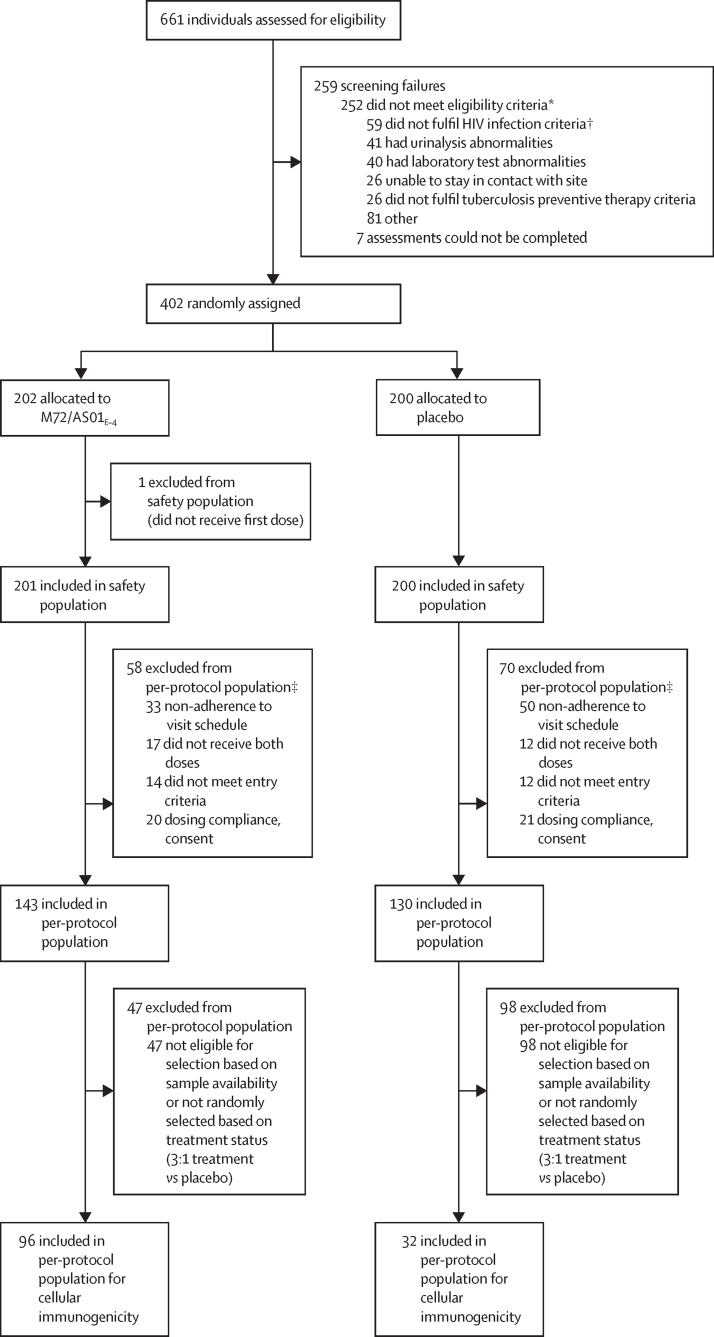
Methods: In this observer-blinded, randomised, controlled, phase 2 trial, participants aged 16-35 years with well controlled HIV were enrolled from urban, semi-urban, and semi-rural settings in South Africa, including sites with high tuberculosis and HIV prevalence, as well as agricultural and mining communities. Participants were randomly assigned (1:1), stratified by site and interferon-gamma release assay (IGRA) status, to receive two intramuscular doses of M72/AS01E-4 or placebo. Eligibility criteria included antiretroviral therapy for at least 3 months, HIV viral load of less than 200 copies per mL, CD4 counts of 200 cells per μL or higher, and previous completion of tuberculosis preventive therapy and no tuberculosis history. The sponsor and its delegates, the laboratory team, investigators, site staff, and participants were blinded to randomisation, whereas an unblinded pharmacist who was not involved in trial procedures prepared placebo and reconstituted M72/AS01E-4 in unit-dose syringes covered with a blinding label. All participants who received at least one dose of either M72/AS01E-4 or placebo were included in the safety population for safety analyses. Immunogenicity analyses were conducted using the per-protocol population, which included participants who received the intervention as planned and did not substantially deviate from the protocol procedures. Safety assessments included solicited adverse events in the first 7 days after each dose, unsolicited adverse events in the first 28 days after each dose, and serious adverse events. Humoral responses were measured with ELISA and cellular responses were assessed using multiparameter flow cytometry, in the per-protocol population. This study is complete and is registered with ClinicalTrials.gov, NCT04556981.
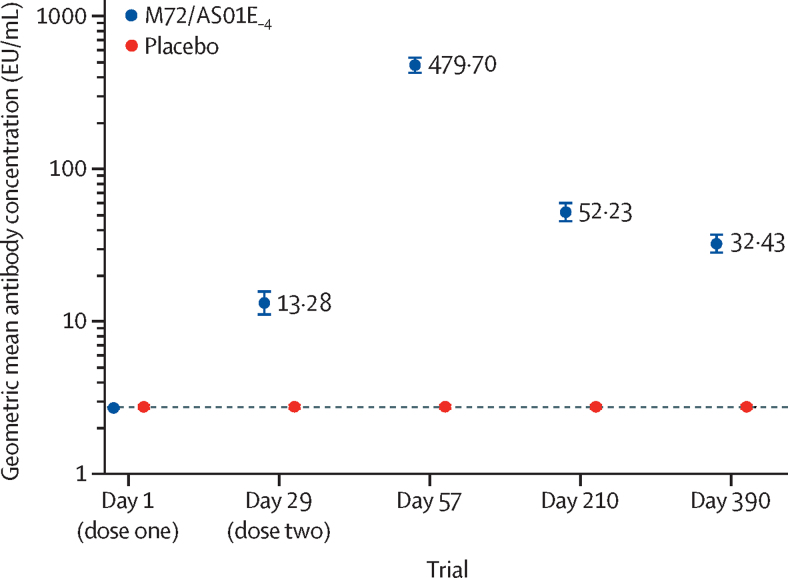
Findings: Between Nov 17, 2020, and Aug 12, 2022, 402 eligible participants were assigned treatment, of whom 401 participants received at least one dose of M72/AS01E-4 (n=201; 175 [87%] were female and 26 [13%] were male; 196 [98%] were Black) or placebo (n=200; [176 [88%] were female and 24 [12%] were male; 196 [98%] were Black) and followed for a median duration of 372 days (IQR 364-389). Among M72/AS01E-4 recipients, solicited adverse events were more frequent, ranging from 17% (33 of 199) for gastrointestinal symptoms to 77% (140 of 183) for injection-site pain. Most events were mild to moderate, with severe events ranging from 0% (0 of 197) for swelling and (0 of 198) redness to 13% (24 of 183) for injection-site pain, resolving within 3 days. Unsolicited adverse events related to vaccine were mainly injection-site reactions in the M72/AS01E-4 group (8% [15 of 201] vs 1% [two of 200] in the placebo group), including erythema, pruritis, swelling, bruising, induration, and pain. No vaccine-related serious adverse events were reported. Among M72/AS01E-4 recipients at day 57 (1 month after dose two), M72-specific antibody geometric mean concentration (GMC) was 479·70 EU/mL (95% CI 421·79-545·56) with median magnitude of CD4 cells of 0·383% (IQR 0·177%-0·663). Among M72/AS01E-4 recipients, at day 57 GMCs were 559·49 EU/mL (95% CI 461·75-677·93) in with baseline IGRA positivity and 424·95 EU/mL (357·74-504·80) in those without; median magnitudes of CD4 cells were 0·447% (IQR 0·287-0·819) and 0·321% (0·147-0·581).
Interpretation: The two-dose regimen of the M72/AS01E-4 tuberculosis vaccine was immunogenic, with an acceptable safety profile. These outcomes led to the inclusion of people living with HIV in the ongoing global registration phase 3 trial.
Funding: Gates Foundation and the Wellcome Trust.
Copyright © 2025 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests At the time this trial was designed, initiated, and conducted, AFD, ACS, LLH, MD, LS, AC, JA, DB, and NF were employees of the Gates Medical Research Institute, and declare no competing interests. RJW receives funding from Wellcome (grant number 226817). He is supported by the Francis Crick Institute, which receives funding from Wellcome (grant number CC2112), UK Research and Innovation (grant number CC2112), and Cancer Research UK (grant number CC2112). He also receives support in part from the National Institute for Health and Care Research Biomedical Research Center of Imperial College National Health Service Trust and received support from the Wellcome Trust and the Gates Foundation to travel to investigator meetings. KM receives funding from the Gates Medical Research Institute (grant number Gates MRI–TBV02–301-DTHF), TB Alliance (grant number NC-009-DTHF), and the National Institutes of Health (grant number UCT00041179, DTHC). She also received travel support from and provided unpaid leadership at the International Union Against Tuberculosis and Lung Disease. LF, JCI, KN, and MT declare no competing interests.
Figures
References
-
- WHO Global Tuberculosis Report. 2023. https://www.who.int/publications/i/item/9789240083851
-
- Lawn SD, Wilkinson RJ. ART and prevention of HIV-associated tuberculosis. Lancet HIV. 2015;2:e221–e222. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
