

Uterine anteroposterior diameter predicts spontaneous pregnancy outcomes in women under 35 years with adenomyosis: a retrospective study
- PMID: 40615802
- PMCID: PMC12228352
- DOI: 10.1186/s12884-025-07828-1
Uterine anteroposterior diameter predicts spontaneous pregnancy outcomes in women under 35 years with adenomyosis: a retrospective study
Abstract
Background: Women diagnosed with adenomyosis often suffer from infertility and frequently seek assisted reproductive techniques (ART). It remains unclear whether certain patients possess the potential to achieve spontaneous pregnancy. This study aimed to investigate the role of uterine parameters, which indicate the progression of adenomyosis, in predicting spontaneous pregnancy outcomes after controlling for other factors that affect natural infertility synergistically.
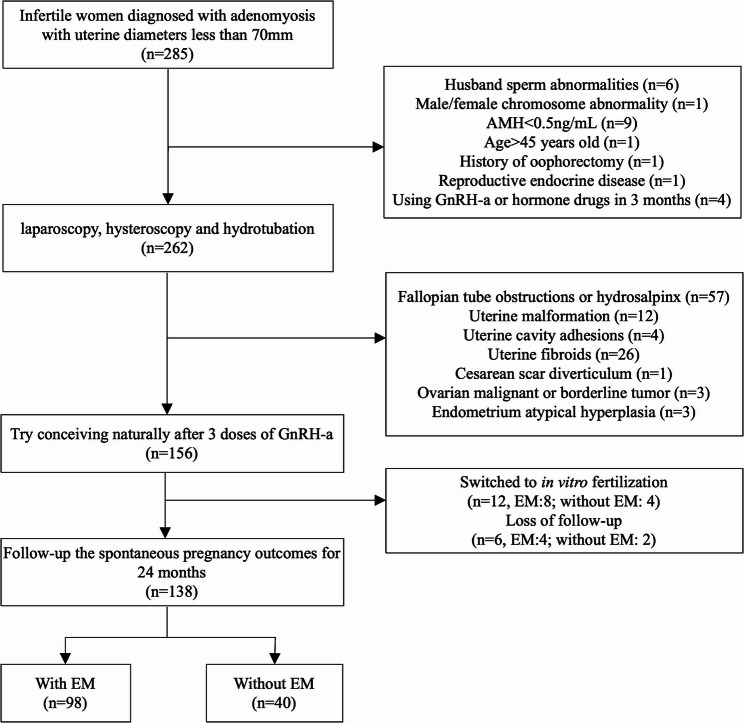
Methods: This retrospective study included 138 infertile women diagnosed with adenomyosis with uterine diameters < 70 mm, who pursued natural conception. Laparoscopy and hysteroscopy were conducted to exclude other factors impacting natural fertility such as hydrosalpinx, and to diagnose and treat endometriosis. The clinical pregnancy rate (CPR) and live birth rate (LBR) within 24 months were compared between patients with endometriosis (n = 98) and those without (n = 40). Logistic regression models were employed to identify predictors of the clinical pregnancy and live birth in both groups, the entire cohort, and subgroups stratified based on age or anti-Müllerian hormone (AMH). Their predictive performance was assessed utilizing receiver operating characteristic (ROC) curves.
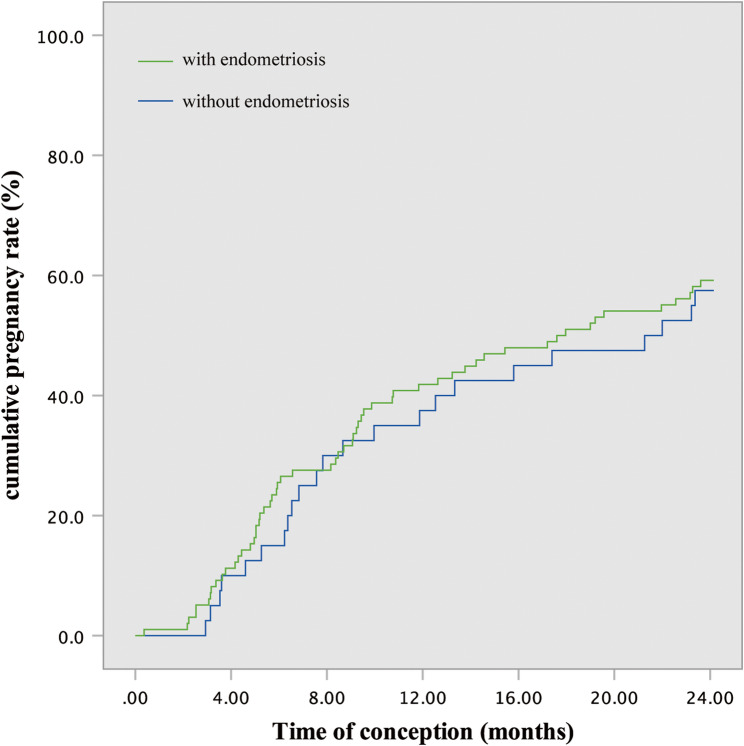
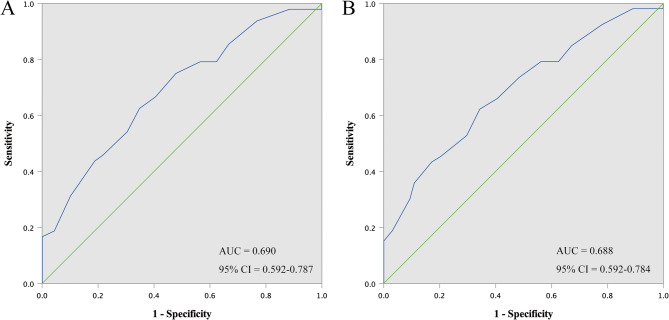
Results: Among the 138 patients, 81 (58.70%) achieved clinical pregnancies, comprising 75 live births (54.35%) and 6 early miscarriages (4.35%). No significant difference was found in CPR or LBR between patients with and without endometriosis. The uterine anteroposterior diameter (AD) predicted pregnancy outcomes in each group and overall. In patients under 35 years, uterine AD independently correlated with successful clinical pregnancy [odds ratio (OR) = 0.878, 95% confidence interval (CI) = 0.814–0.946] and live birth (OR = 0.884, 95% CI = 0.821–0.951). A uterine AD of < 41.5 mm predicts successful clinical pregnancy [sensitivity: 0.625, specificity: 0.652, area under the curve (AUC): 0.690] and live birth (sensitivity: 0.623, specificity: 0.656, AUC: 0.688).
Conclusion: Uterine AD predicted spontaneous pregnancy outcomes in patients under 35 years diagnosed with adenomyosis. Adenomyosis probably compromises fertility from the early stages of the condition. However, the retrospective design, the potential presence of confounding factors and limited sample size of this study indicate the necessity for large-scale prospective studies to validate these findings.
Keywords: Adenomyosis; Endometriosis; Hysteroscopy; Laparoscopy; Pregnancy outcome.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, and was approved by the ethics committee of the Obstetrics and Gynecology Hospital of Fudan University (Code: 2024 − 148). The verbal informed consent was obtained from all patients by telephone connection. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
