

Clinical characteristics of AATD-related COPD patients vary with age at diagnosis: data from the EARCO international registry
- PMID: 40616025
- PMCID: PMC12231694
- DOI: 10.1186/s12890-025-03782-y
Clinical characteristics of AATD-related COPD patients vary with age at diagnosis: data from the EARCO international registry
Abstract
Background: This study aims to evaluate the clinical characteristics of COPD patients with AATD according to their age at diagnosis.
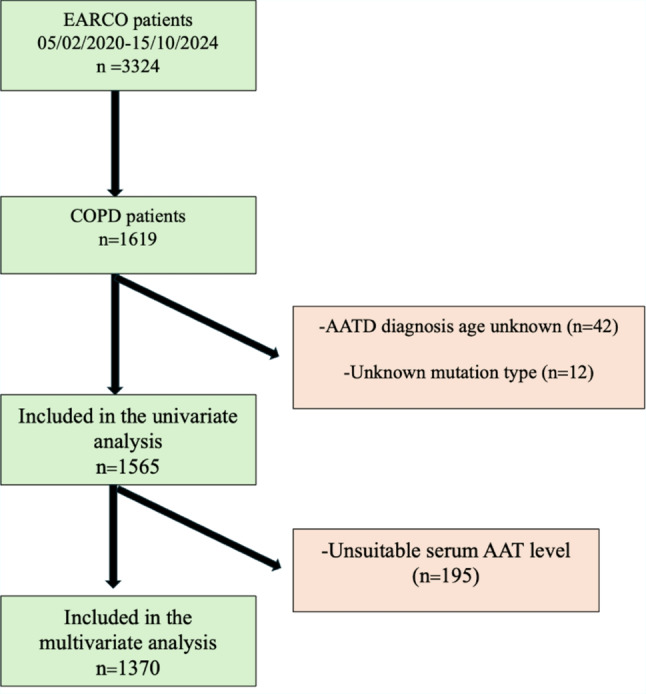
Methods: Data was obtained from the European Alpha-1 Research Collaboration (EARCO) registry, an international prospective cohort study. AATD patients with COPD registered between February 2020 and October 2024 were analysed. Clinical charateristics were compared between groups, stratified by age of AATD diagnosis as follows; <45, 45-65 and ≥65 years. A multivariable logistic regression model explored factors associated with age at diagnosis.
Results: A total of 1,565 AATD-COPD patients were included, with 18.2% receiving an AATD diagnosis at age ≥ 65. In univariate comparisons according to diagnosis age revealed that the prevalence of patients with Pi*ZZ mutation was lower in the ≥ 65 age group (47.1%) compared to the 45-65 (65.5%) and < 45 (78.5%) age groups. In contrast, the prevalence of Pi*SZ and Pi*SS were higher in the ≥ 65 group compared to the younger age groups. The proportion of never-smokers was highest in the ≥ 65 group (39.5%), whereas only 15.3% of patients under 45 were never-smokers. Multivariate analysis showed that; compared to never-smokers, former smoking (OR: 0.08; 95% CI: 0.03-0.23) and current smoking (OR: 0.43; 95% CI: 0.27-0.70) were negatively associated with a diagnosis at age ≥ 65 in all sample. Compared to the Pi*ZZ genotype, among all sample, Pi*SS was associated with more than a 3-fold increased likelihood of diagnosis at age ≥ 65 and when considering only index cases Pi*SZ was associated with diagnosis age of ≥ 65 (OR: 2.01, 95%CI: 1.01-4.04). Among patients with the Pi*ZZ, current smoking was negatively associated (OR:0.24,95%CI: 0.13-0.47) with a diagnosis at age ≥ 65, whereas higher FEV1% and serum AAT levels were positively associated with later diagnosis.
Conclusion: Patients diagnosed at an older age had lower tobacco exposure and less severe disease. This suggests that subclinical symptoms may contribute to delays in diagnosis, as COPD features can be subtle or under-recognised until later in life. Our findings highlight the importance of considering AATD in all COPD patients, regardless of age, to avoid missed or delayed diagnoses.
Keywords: AATD; COPD; Diagnosis age; Elderly.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol received central ethical approval from the Research Ethics Committee of the Vall d’Hebron University Hospital, Barcelona, Spain (PR(AG)480/2018) and was subsequently approved by all participating centres. Also every participating center obtained ethical approval from coordinating centers of the country. For Türkiye (corresponding author’s country) from Manisa Celal Bayar University Medical Faculty Clinical Researches Ethical Committee Approval number 39, Date: 06.08.2019 and for EARCO exacerbation study from Recep Tayyip Erdoğan University Clinical Researches Ethical Committee Approval number:274, Date: 12.06.2024. Informed consent was obtained from all participants. This study was completed in accordance with the Helsinki Declaration as revised in 2013. Consent for publication: Written informed consent was obtained from the patients described herein for their anonymized information to be published in this article. Competing interests: Catarina Guimarães has received speaker fees from CSLBehring. María Torres-Durán has received either speaker and consulting fees from CSL Behringand Grifols, and support for attending meetings from CSL Behring, Grifols, Chiesi and FAESFarma. Alice M Turner has received either grants or speaker fees from AstraZeneca,GlaxoSmithKline, Boehringer Ingelheim, Chiesi, CSL Behring, Takeda, Vertex and GrifolsBiotherapeutics. Hanan Tanash has received speaker fees from AstraZeneca, GlaxoSmithKline,Boehringer Ingelheim, Chiesi and Grifols. Carlota Rodríguez-García has received speaker feesfrom AstraZeneca, GlaxoSmithKline, Grifols, Chiesi, and CSL Behring, expert testimony for Chiesi,support for attending meetings from Chiesi and Grifols. Angelo Corsico has received speakerfees and honoraria for participation on advisory board from CSL Behring, and honoraria formanuscript writing from Grifols. JoséLuis López-Campos has received honoraria during the last3 years for lecturing, scientific advice, participation in clinical studies or writing for publications for (alphabetical order): AstraZeneca, Bial, Boehringer, Chiesi, CSL Behring, Faes, Gebro, Grifols, GSK, Menarini, Sanofi, Zambon. Juan Luis Rodríguez-Hermosa has received honoraria during the last 3 years for lecturing, scientific advice or participation in clinical studies from AstraZeneca, Bial, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, Grifols and Zambon. JoséMaría Hernández-Pérez has received consulting fees from Grifols and CSL Behring, speaker fees from AstraZeneca, Bial, CSL Behring, FAES laboratory, GlaxoSmithKline, and Grifols, support for attending meetings from Grifols and CSL Behring, and honoraria for participation on advisory board from Grifols. Maria Sucena has received consulting fees from Bial, GSK, CSL Behring Grifols and Sanofi, speaker fees from AstraZeneca, Bial, CSL Behring, GSK and Grifols. Paul Ellis has received speaker frees from Chiesi, Astra Zeneca, GSK and Takeda. The remaining authors report no conflicts of interest.
Figures



References
-
- Stoller JK. Detecting Alpha-1 Antitrypsin Deficiency: Current State, Impediments, Opportunities, and Future Directions. Ann Am Thorac Soc. 2024 Sep 23. 10.1513/AnnalsATS.202406-600FR. Epub ahead of print. PMID: 39311761. - PubMed
-
- Miravitlles M, Dirksen A, Ferrarotti I, Koblizek V, Lange P, Mahadeva R, McElvaney NG, Parr D, Piitulainen E, Roche N, Stolk J, Thabut G, Turner A, Vogelmeier C, Stockley RA. European Respiratory Society statement: diagnosis and treatment of pulmonary disease in α1-antitrypsin deficiency. Eur Respir J. 2017;50(5):1700610. 10.1183/13993003.00610-2017. PMID: 29191952. - PubMed
-
- Calle Rubio M, Soriano JB, López-Campos JL, Soler-Cataluña JJ, Alcázar Navarrete B, Rodríguez González-Moro JM, Miravitlles M, Barrecheguren M, Fuentes Ferrer ME, Rodriguez Hermosa JL, EPOCONSUL Study. Testing for alpha-1 antitrypsin in COPD in outpatient respiratory clinics in Spain: A multilevel, cross-sectional analysis of the EPOCONSUL study. PLoS One. 2018;13(6):e0198777. 10.1371/journal.pone.0198777. Erratum in: PLoS One. 2019;14(2):e0212522. doi: 10.1371/journal.pone.0212522. PMID: 29953442; PMCID: PMC6023216. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
