

Work-related musculoskeletal disorders and associated factors among hospital sanitary workers in public hospitals of Eastern Ethiopia
- PMID: 40616057
- PMCID: PMC12226844
- DOI: 10.1186/s12891-025-08873-9
Work-related musculoskeletal disorders and associated factors among hospital sanitary workers in public hospitals of Eastern Ethiopia
Abstract
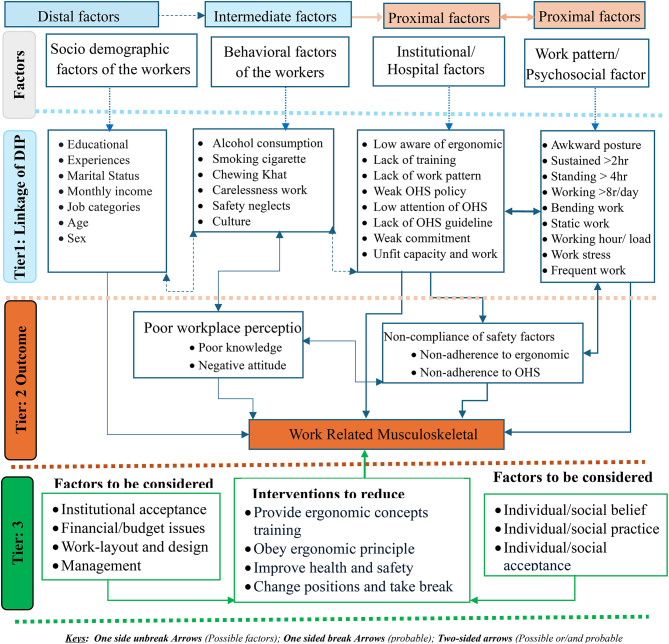
Introduction: Work-related Musculoskeletal disorders (WMSDs) are serious problems of public health at health care facilities that reduce health quality of the workers. These issues arise from poor work design, unsafe and unhygienic conditions, lack of ergonomic practices, and inadequate occupational health and safety (OHS) services, which are common in low-middle-income countries, which remain underexamined among hospital sanitation workers (SWs) in eastern Ethiopia.
Objective: This study aimed to assess WMSDs and associated factors among public hospital SWs in eastern Ethiopia.
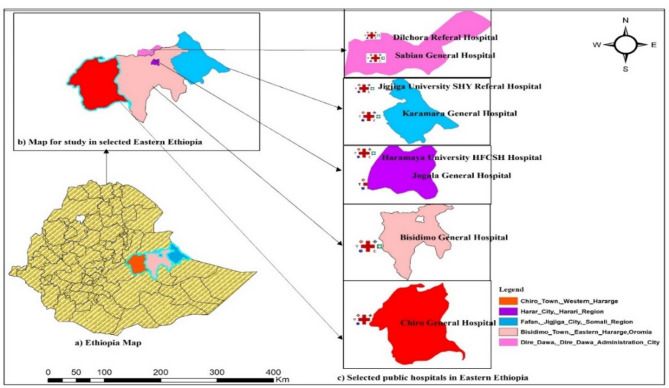
Methods: Hospital based cross sectional study was conducted in eastern Ethiopia in 2023. A well-structured questionnaire prepared. The internal consistency (α value) for the prepared questions was 0.95. Simple random sampling was used to choose eight hospitals among a total of fourteen public hospitals in these areas. A single proportion formula long with design effect of 2.0 and 5% of non-response rate was calculate the sample size and obtained 791 SWs, which is approaching actual number of SWs within selected hospitals. Thus, all (809) of SWs were recruited for the study. Face-to-face interview was conducted. Epi Data version 3.1 was used for data entry and Stata version 17MP was used for the data analysis. Data quality was ensured through training of data collectors, language translation, pretesting, and adjusting for confounders. The robust Modified Poisson/MP regression was used to identify predictors of WMSDs. Bi-variate MP model was used to perform un-adjusted prevalence ratio (UPR). While, MP multi-variable was used to analysis the adjusted prevalence ratio (APR) for predictors with significant values of p ≤ 0.20. The results were deemed statistically significant at the two-tailed level with a 95% confidence interval (CI:95%) and a p-value of 0.05. Finally, seven variables those have ≤ p-value 0.05 at APR were candidate for Structural equation modeling (SEM) to estimate the correction and direction of risk factors for WMSDs.
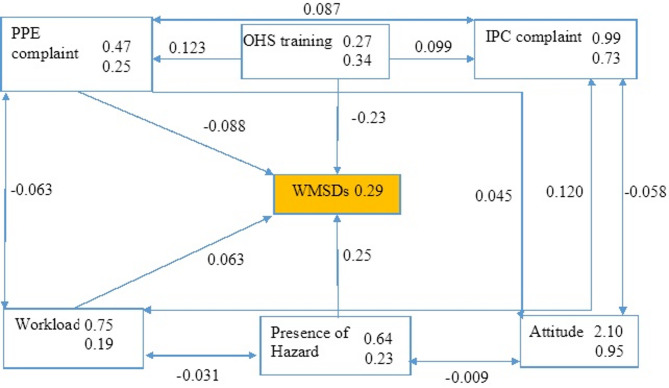
Result: Out of a total of 809 SWs, 729 (90.11%) of them responded. The current study found self-reported WMSDs among SWs was 51.17% (95% CI: 0.48, 0.55). Multivariable MP regression model shows that SWs with acquired diseases (APR: 1.85; 95% CI: 1.62, 2.12), SWs with occupational injuries (APR: 1.16, 95% CI: 1.04, 1.33) and those exposed with occupational hazards (APR:1.42; 95% CI: 1.18, 1.70) were more likely to report WMSDs. Similarly, those didn't get health and safety training (APR:1.20; 95% CI: 1.03, 1.43), those had workload (APR: 1.36; 95% CI: 1.05, 1.76) and non-adhered to personal protective equipment [PPE] (APR: 1.17; 95% CI: 1.00, 1.38) were more likely to report high WMSDs. SEM found that hazards exposures (β = 0.25; 95% CI: 0.18, 0.33) and workload (β = 0.06; 95% CI: 0.03,0.15) were positive correlations. While, compliance with PPE (β= -0.09; -0.16, -0.01) and provide OHS training (β= -0.23; 95% CI: -0.342, -0.03) have negative correlation with WMSDs (p-value < 0.05).
Conclusion: The study found that more than half of SWs were suffered with WMSDs. The main attributed risk factors were poor work conditions, lack of ergonomic applications, a lack of institutional supports, and behavioral factors. Thus, the study highlights the critical policy requirement to enhance ergonomic application and health and safety improvement in order to lower WMSDs. The hospitals should provide interventions such as training on ergonomic concepts, adapt the guideline and adhere the ergonomic policies and regulations. Federal ministry of health and Federal ministry of labor and social affairs should cooperatively set standards, support and monitoring compliance, provide resources and enforce protocols in order to lower WMSDs among these vulnerable work-forces.
Keywords: Ergonomics; Occupational health; Public hospitals; Sanitation workers; Work-related musculoskeletal disorders.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The authors declare the consent of the study was obtained from Haramaya University College of Health and Medical Sciences “Institutional Health Research Ethics Review Committee” (Ref: IHRERC/064/2023. Then the formal letter was written to each hospital. Then, informed consent was obtained from the hospitals to verify their willingness to participate in the study. All study participants were signed written form in order to participate on the study. The confidentiality of the individuals was upheld in compliance with the Helsinki Protocol, a collection of moral guidelines for human subject’s medical research. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Co-occurrence of occupational outcomes and associated factors among hospitals cleaners, eastern ethiopia: a cross sectional study.BMC Public Health. 2024 Nov 11;24(1):3108. doi: 10.1186/s12889-024-20571-0. BMC Public Health. 2024. PMID: 39529077 Free PMC article.
-
Occupational health risk perceptions and determinants: knowledge and attitude of sanitary workers in public hospitals of Ethiopia.Front Public Health. 2025 May 9;13:1509595. doi: 10.3389/fpubh.2025.1509595. eCollection 2025. Front Public Health. 2025. PMID: 40416666 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
Work-related musculoskeletal disorders and associated factors among workers in Kombolcha Textile Industry, Northeast Ethiopia.Sci Rep. 2025 Jul 19;15(1):26260. doi: 10.1038/s41598-025-10775-8. Sci Rep. 2025. PMID: 40683931 Free PMC article.
References
-
- Doğrul Z, Mazican N, Turk AM. The prevalence of work-related muskuloskeletal disorders and related factors among occupational disease clinic patients. Int Arch Public Health Community Med. 2019;3(2):01–7. 10.23937/2643-4512/1710030
-
- Iñigo I. IKEI: Work-related musculoskeletal disorders – Facts and figures synthesis report 10 EU member states reports. 2020. Available at: https://osha.europa.eu/sites/default/files/Work-related_MSDs_prevalence_...
-
- Da Costa B, Vieira E. Risk factors for work-related musculoskeletal disorders: a systematic review. Am J Ind Med. 2010;53(3285–323) 10.1002/ajim.20750 - PubMed
-
- Lin X, Xu Y, Xu J, Pan X, Song X, Shan L, Zhao Y, Shan. Global burden of noncommunicable disease. Endocr. 2020;69(2):310–20. 10.1007/s12020-020-02352-y - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
