

Incidence and prevalence of ANCA-associated vasculitis in Oslo, Norway, applying different criteria-based case definitions: a population-based cohort study
- PMID: 40617587
- PMCID: PMC12228444
- DOI: 10.1136/rmdopen-2025-005526
Incidence and prevalence of ANCA-associated vasculitis in Oslo, Norway, applying different criteria-based case definitions: a population-based cohort study
Abstract
Objective: To provide complete data on the incidence and prevalence of antineutrophil cytoplasmic antibody-associated vasculitides (AAV) over the years 2000-2016 in the Oslo area, Norway, with 528 924 adults (aged 18+) in 2016.
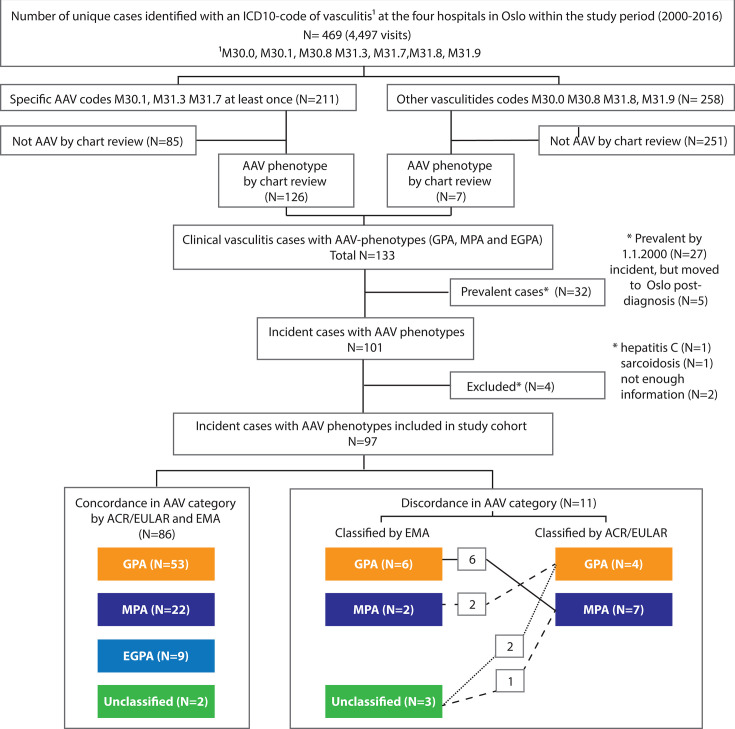
Methods: From administrative databases, we identified all cases with International Classification of Disease, 10th Revision (ICD-10) codes indicative of necrotising small vessel vasculitis during 2000-2016 in the Oslo area. We manually chart reviewed every case identified through the ICD-10 search to confirm (or reject) a clinical AAV diagnosis. Cases with confirmed clinical AAV were classified by the European Medicine Agency (EMA) algorithm and the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR 2022) classification criteria.
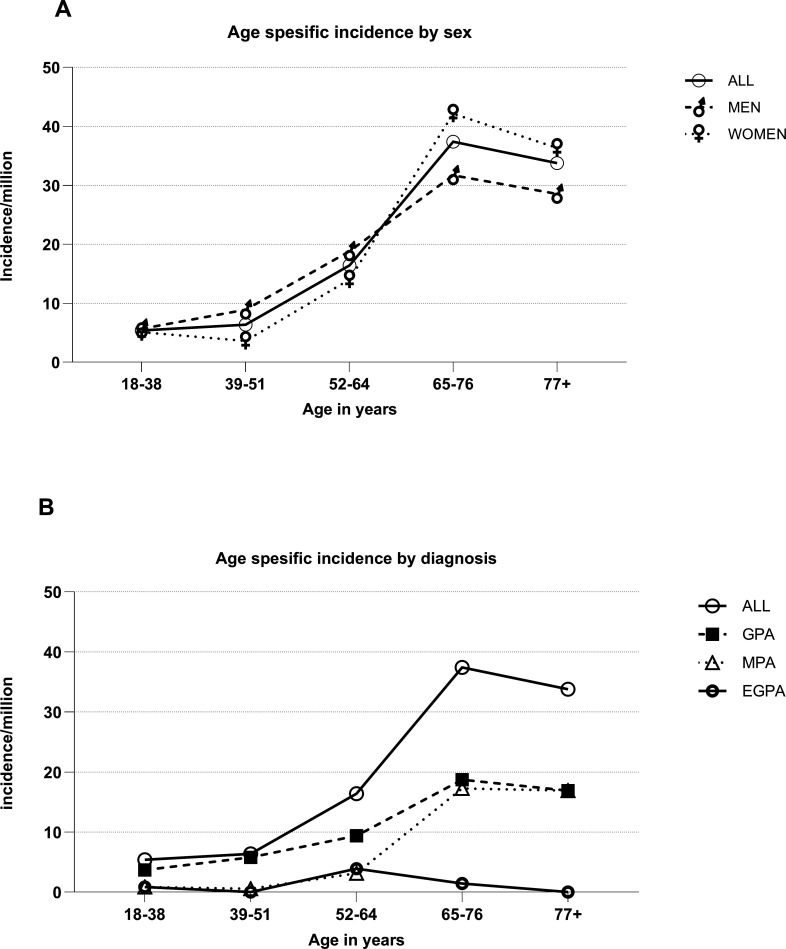
Results: Among 469 cases with an ICD-10 code indicative of small vessel vasculitis, chart review confirmed AAV in 133 cases with 97 having new onset during the study. Of these 97 incident cases, 57 (60%) were classified as granulomatosis with polyangiitis (GPA), 29 (31%) as microscopic polyangiitis (MPA) and 9 (9%) as eosinophilic granulomatosis with polyangiitis (EGPA) per ACR/EULAR 2022 criteria, while 2 remained unclassified. There was an 11% discordance in AAV case classification between the 2022 criteria and the EMA algorithm. The mean annual incidence of AAV in adults was 12.2 per million (7.3 for GPA, 3.7 for MPA and 1.2 for EGPA). Across the study period, incidence rates increased numerically, and prevalence peaked at 143.7 AAV cases/million adults in 2016.
Conclusion: This population-based study adds new evidence that AAV increases in Europe and indicates that using the ACR/EULAR 2022 criteria shifts cases from GPA to MPA relative to the EMA algorithm, affecting epidemiology estimates.
Keywords: Classification; Epidemiology; Incidence; Prevalence; Systemic vasculitis.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Performance of EMA algorithm, 2022 ACR/EULAR criteria, and EMA-ACR/EULAR algorithm in classifying pediatric ANCA-associated vasculitis: a national cohort study in China.World J Pediatr. 2025 Apr;21(4):372-385. doi: 10.1007/s12519-025-00899-2. Epub 2025 May 10. World J Pediatr. 2025. PMID: 40347428 Free PMC article.
-
The role of tobacco smoking in anti-neutrophil cytoplasmic antibody-associated vasculitis: a systematic review.Clin Exp Rheumatol. 2024 Jul;42(7):1321-1332. doi: 10.55563/clinexprheumatol/nu8ngr. Epub 2024 Jul 4. Clin Exp Rheumatol. 2024. PMID: 38976289
-
Incidence of anti-neutrophil cytoplasmic antibody-associated renal vasculitis: a retrospective study in rural and regional Victoria, Australia.Intern Med J. 2024 Mar;54(3):461-466. doi: 10.1111/imj.16127. Epub 2023 May 29. Intern Med J. 2024. PMID: 37183767
-
Efficacy of plasma exchange for antineutrophil cytoplasmic antibody-associated systemic vasculitis: a systematic review and meta-analysis.Arthritis Res Ther. 2021 Jan 14;23(1):28. doi: 10.1186/s13075-021-02415-z. Arthritis Res Ther. 2021. PMID: 33446268 Free PMC article.
-
Comparison of the 2022 ACR/EULAR Classification Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Previous Criteria.Yonsei Med J. 2023 Jan;64(1):11-17. doi: 10.3349/ymj.2022.0435. Yonsei Med J. 2023. PMID: 36579374 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials