

Clinical patterns and predictors of trauma-related mortality over 13 years: a retrospective analysis from a Level 1 National trauma center
- PMID: 40618106
- PMCID: PMC12229009
- DOI: 10.1186/s13017-025-00633-3
Clinical patterns and predictors of trauma-related mortality over 13 years: a retrospective analysis from a Level 1 National trauma center
Abstract
Background: Qatar is one of six neighboring countries in the Gulf Cooperation Council region that form a political and economic alliance to foster multilateral cooperation. Given the shared challenges in trauma care, there is a need for a collaborative network to develop region-specific injury prevention strategies. For example, this study examines the clinical patterns and predictors of hospital mortality among trauma patients in Qatar.
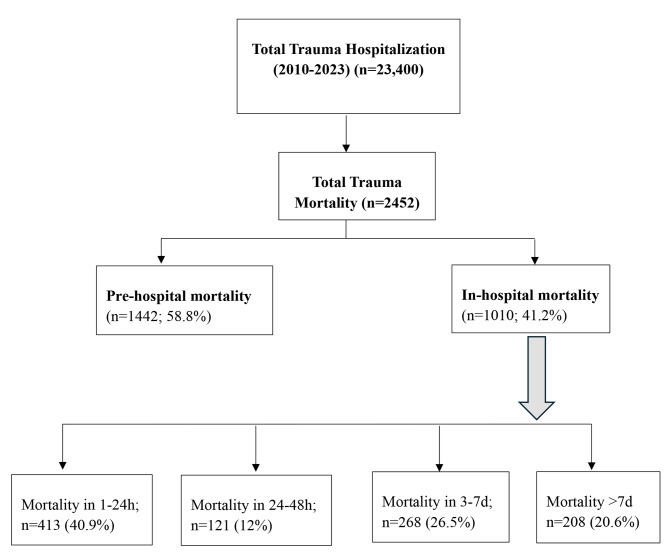
Methods: A retrospective analysis of trauma-related deaths (2010-2023) was conducted. Patients were stratified into early hospital mortality (EHM, ≤ 48 h) and late hospital mortality (LHM, > 48 h) groups. Further analyses examined in-hospital mortality (24 h, 24-48 h, 3-7 days, and > 7 days), age groups, injury mechanisms, and severity. A multivariable regression analysis identified predictors of early mortality.
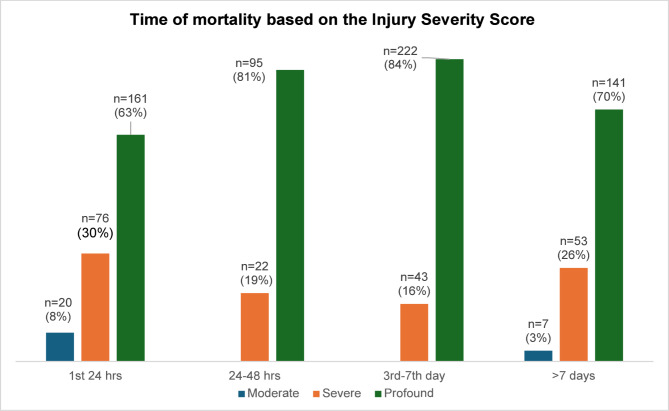
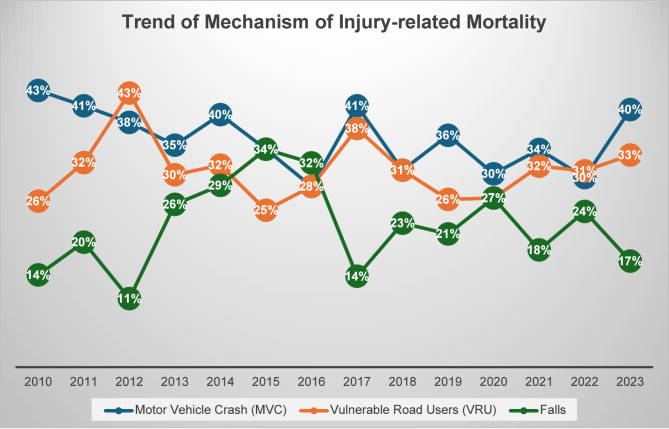
Results: Among 2,452 trauma-related deaths, 59% occurred in pre-hospital, while 41% occurred in-hospital. Compared to LHM (47%), EHM (53%) was associated with a younger age (35 vs. 39 years; p = 0.002), higher systolic blood pressure (0.82 vs. 0.67; p = 0.002), and diastolic blood pressure (2.03 vs. 1.75; p = 0.001). Motor vehicle crash (MVC) was the leading cause of death (35.3%), with vulnerable road users (VRU) the commonest in EHM (p = 0.004) and falls in LHM (p = 0.004). LHM was associated with a higher injury severity score (p = 0.001). On-admission systolic shock index independently predicted EHM (OR 2.23; 95% CI 1.09-4.52), while head (OR 7.14; 95% CI 2.44-20.00) and pelvic injuries (OR 3.70; 95% CI 1.19-11.11) and sepsis (OR 6.25; 95% CI 1.22-33.33) predicted LHM. In-hospital deaths exhibited a bimodal distribution, with peaks at 24 h (15%) and between the third and seventh days (10%). EHM showed an upward trend over the years (R² = 0.312), while LHM remained stable. Trauma-related mortality rates declined from 10.4 to 5.0 per 100,000 population (2011 and 2017) before rising to 9.7 by 2022. Pre-hospital deaths followed a similar pattern to the overall mortality, while the in-hospital rates remained steady. VRU-related injuries persisted at a high level, accounting for 26-43% of cases throughout the study period.
Conclusion: This study highlights distinct trauma-related mortality patterns, with EHM linked to hemorrhage and shock, while LHM is associated with severe head injuries and sepsis. These findings underscore the need for targeted interventions to optimize bleeding control and address predictors such as shock indices for EHM and head injuries for LHM.
Keywords: Early death; In-hospital; Injury predictors; Mortality; Pre-hospital; Trauma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was obtained from the institutional review board (MRC 12263/12 & 01/18/330 & 01/23/671) at the Medical Research Center, Hamad Medical Corporation (HMC), Doha, Qatar. Data was collected retrospectively and anonymously with no direct contact with the patients; therefore, a waiver of consent was granted. Consent for publication: not applicable. Competing interests: The authors declare no competing interests. Conflict of interest: none.
Figures


References
-
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–61. - PMC - PubMed
-
- Forrester JD, August A, Cai LZ, Kushner AL, Wren SM. The golden hour after injury among civilians caught in conflict zones. Disaster Med Public Health Prep. 2019;13(5–6):1074–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
