

Exploring Different Levels of Contact Frequency in Multiple Sclerosis Care
- PMID: 40619983
- PMCID: PMC12230343
- DOI: 10.1002/brb3.70634
Exploring Different Levels of Contact Frequency in Multiple Sclerosis Care
Abstract
Introduction: Previous studies have identified differences in healthcare contacts, needs, and cost of care among persons living with multiple sclerosis (MS). The need for a deeper understanding of factors influencing healthcare contacts has been highlighted. The aim of this study was to explore different levels of healthcare contact frequency among persons living with MS.
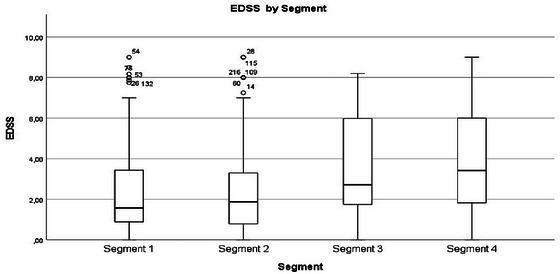
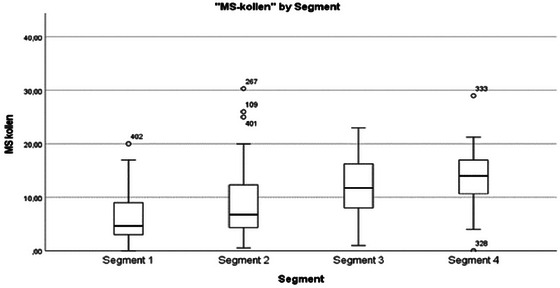
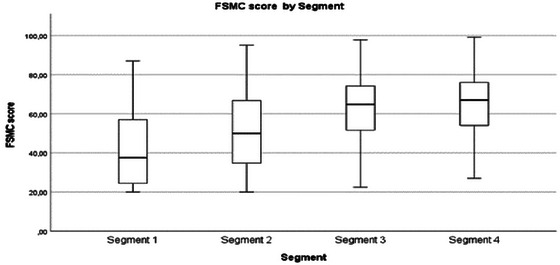
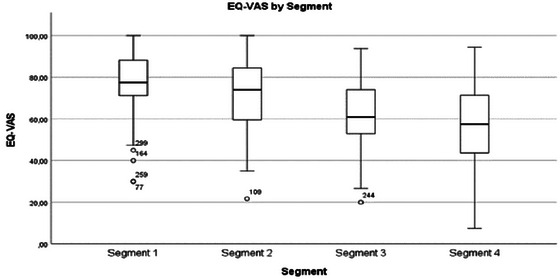
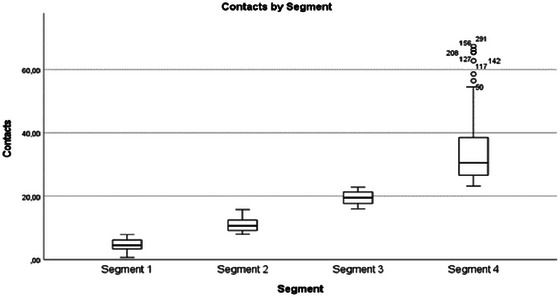
Method: Both quantitative and qualitative data were collected, analyzed, and integrated in a parallel mixed-methods approach with data integration through joint display. Data were retrieved from the hospital administrative system, the Swedish national MS registry, and a previously conducted interview study. The population was divided into four segments based on healthcare contact frequency, ranging from Segment 1, with the fewest visits, to Segment 4, representing those with the most frequent contacts. Analyses were conducted using descriptive statistics, statistical tests on differences between segments, multinomial logistic regression, deductive content analysis, and integration.
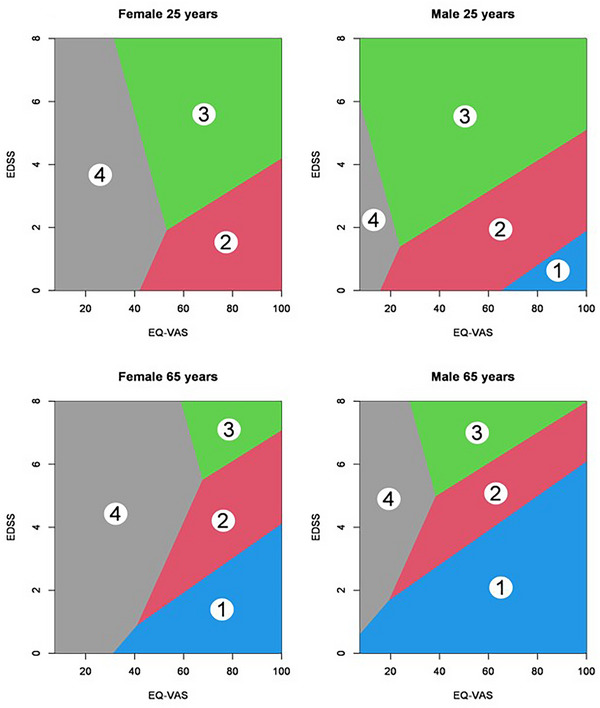
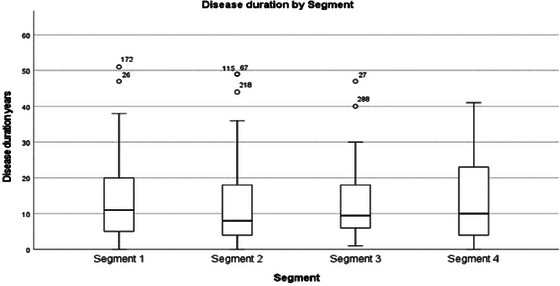
Results: The mean and median distribution of individual study variables increased or decreased (depending on scale direction) between segments for most variables toward more symptoms, reduced function, and declining experiences of health from the lowest to the highest contact frequency. The probability of belonging to a certain segment was influenced by the explanatory variables age, gender, overall health, and expanded disability status with the different variables playing different roles for each segment. Qualitative findings also suggested increased physical limitations with increased level of healthcare contacts. This was not necessarily due to MS and influence of comorbidities was sometimes expressed. Both requests of less and more healthcare contacts existed and content of healthcare contacts could have more personalized design overall, health care was perceived positively across all segments. Data integration with merged interpretation included eight themes, characteristics of the population, neurological assessment and gait function, symptoms and consequences, fatigue and cognition, perspectives on health, examinations, interactions with health care, and disease duration and future. The merged interpretation confirmed patterns of symptoms, reduced function, and declining experiences of health from the lowest to the highest contact frequency and expanded on individual variation within segments and influenced by comorbidities. Discord in data regarded relations with others, aspects of medication, and knowledge building and type of MS.
Conclusion: The findings on distribution of variables and experiences across segments, were increase in symptoms, loss of function, and deterioration of health experience correlating with increased levels of contact frequency from Segments 1 to 4. The explanatory variables found were age, gender, overall health, and expanded disability. The merged interpretation, expand on individual differences on how symptoms were experienced and influenced by comorbidities. Discord found, regarding for example personal context and aspects of self-care where areas that may be overlooked in healthcare contacts. The explanatory variables identified in this study are suggested to be further explored together with the knowledge of persons living with MS and professionals.
Keywords: care contacts; contact frequencies; multiple sclerosis care.
© 2025 The Author(s). Brain and Behavior published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Allison, P. D. 2012. Logistic Regression Using SAS: Theory and Application. 2nd ed. SAS Institute.
-
- Baert, P. 2004. “Pragmatism as a Philosophy of the Social Sciences.” European Journal of Social Theory 7, no. 3: 355–369. 10.1177/1368431004044198. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
