

Long-term Outcomes of a Contemporary Arthroscopic Bankart Repair Technique in Patients With Traumatic Anterior Shoulder Instability: A Minimum 10-Year Follow-up
- PMID: 40620132
- PMCID: PMC12311240
- DOI: 10.1177/03635465251351293
Long-term Outcomes of a Contemporary Arthroscopic Bankart Repair Technique in Patients With Traumatic Anterior Shoulder Instability: A Minimum 10-Year Follow-up
Abstract
Background: The long-term results of arthroscopic Bankart repair are poorly reported in the literature and show recurrence rates as high as 37%. However, this high failure rate is based on historical studies of patients with critical defects stabilized using older techniques.
Purpose: To evaluate the long-term clinical outcomes of arthroscopic Bankart repair using a contemporary technique with a minimum of 3 suture anchors in patients with traumatic anterior instability and to assess possible risk factors for recurrent instability.
Study design: Case series; Level of evidence, 4.
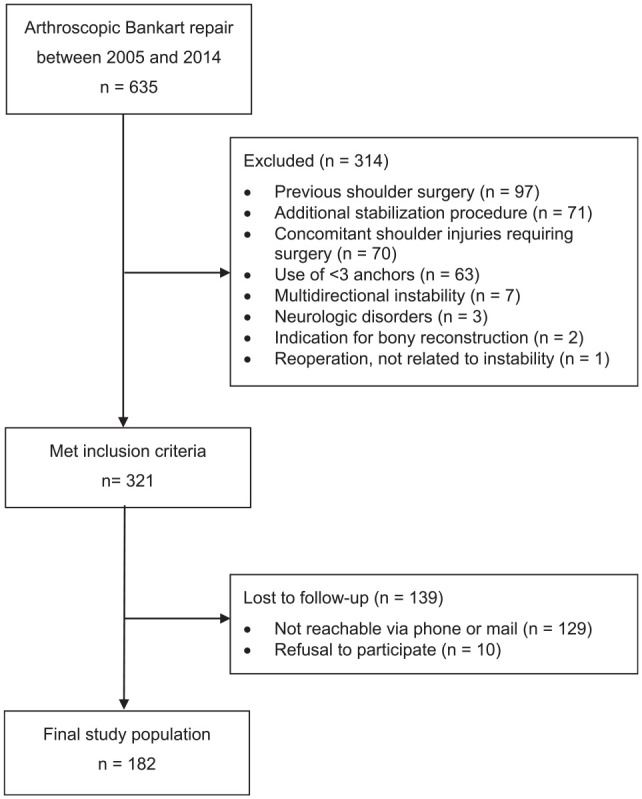
Methods: A total of 181 patients (182 shoulders), who underwent arthroscopic Bankart repair because of traumatic anterior instability between 2005 and 2014, were included in this study and evaluated at a minimum follow-up of 10 years. Exclusion criteria were previous shoulder surgery, additional stabilization procedures, use of <3 anchors, multidirectional instability, and indications for bony reconstruction (critical bony defects: glenoid defect >20%, off-track Hill-Sachs lesion). The primary outcome was recurrent instability. Secondary outcomes were the Subjective Shoulder Value (SSV), visual analog scale (VAS), Constant score, Western Ontario Shoulder Instability Index (WOSI), and Rowe score as well as sports activity level and return to sports. Risk factors for recurrent instability were analyzed.
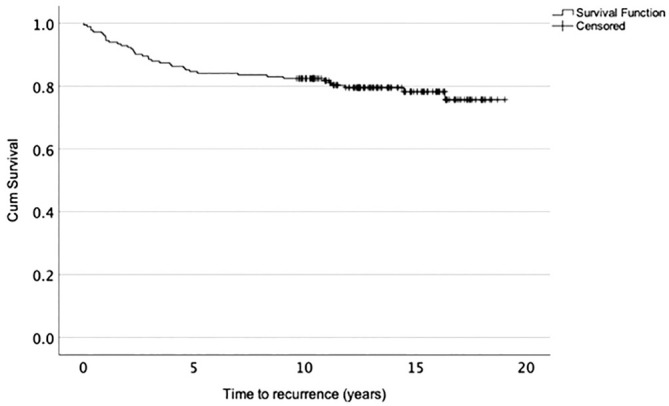
Results: The overall recurrence rate was 20.9% at a mean follow-up of 13.8 ± 2.8 years. Age ≤20 years at the time of surgery was associated with a higher risk of recurrence (P = .007). The failure rate was lower in patients who underwent surgery after the first-time dislocation (8/58 [13.8%]) compared with patients who underwent surgery after multiple instability events (30/124 [24.2%]), although this was not statistically significant (P = .108). Patients without recurrent instability had statistically significant better scores on the SSV (P < .001), VAS for pain during movements (P = .016), Constant score (P = .011), WOSI (P = .001), and Rowe score (P < .001) compared with patients with recurrence without revision surgery. A shorter interval between the first dislocation and surgery was associated with better shoulder outcomes, despite a consistent recurrence rate. Of all patients, 97.6% returned to sports, with 69.6% returning to 90% to 100% of their preoperative sports activity.
Conclusion: Arthroscopic Bankart repair resulted in a relatively high recurrence rate, despite the use of a contemporary technique, particularly in patients with >1 dislocation before surgery. While younger age and a higher number of preoperative dislocations were potential risk factors for recurrence, a shorter interval between the first dislocation and surgery was associated with improved clinical outcomes. Therefore, patients with a high risk of redislocations should be considered for early soft tissue stabilization, while additional procedures such as remplissage should be performed for those with nonmodifiable high-risk factors.
Keywords: Bankart repair; arthroscopic surgery; recurrence rate; shoulder instability.
Conflict of interest statement
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Aboalata M, Plath JE, Seppel G, Juretzko J, Vogt S, Imhoff AB. Results of arthroscopic Bankart repair for anterior-inferior shoulder instability at 13-year follow-up. Am J Sports Med. 2017;45(4):782-787. - PubMed
-
- Balg F, Boileau P. The Instability Severity Index Score: a simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007;89(11):1470-1477. - PubMed
-
- Bankart ASB. The pathology and treatment of recurrent dislocation of the shoulder-joint. Br J Surg. 1938;26(101):23-29.
-
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part III: the SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy. 2003;19(6):641-661. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
