

Management of Osilodrostat Therapy in Patients With Cushing's Syndrome: A Modified Delphi Consensus Panel
- PMID: 40620482
- PMCID: PMC12227144
- DOI: 10.1210/jendso/bvaf103
Management of Osilodrostat Therapy in Patients With Cushing's Syndrome: A Modified Delphi Consensus Panel
Abstract
Introduction: Endogenous Cushing's syndrome (CS) is a rare endocrine disorder that chronically exposes patients to supraphysiological cortisol levels. Primary therapy for CS consists of surgery. Medical therapies are also considered for many patients with CS, including those who are not surgical candidates or have persistent or recurrent hypercortisolism after surgery. Osilodrostat, an adrenal steroidogenesis inhibitor, demonstrated sustained efficacy and safety in phase 3 clinical trials and is currently approved to treat endogenous CS in Europe and the United States. Because of limited clinical experience, questions remain about how to individualize osilodrostat treatment for different clinical scenarios and special populations. Additional guidance from experts based on clinical study and real-world experiences with osilodrostat is needed.
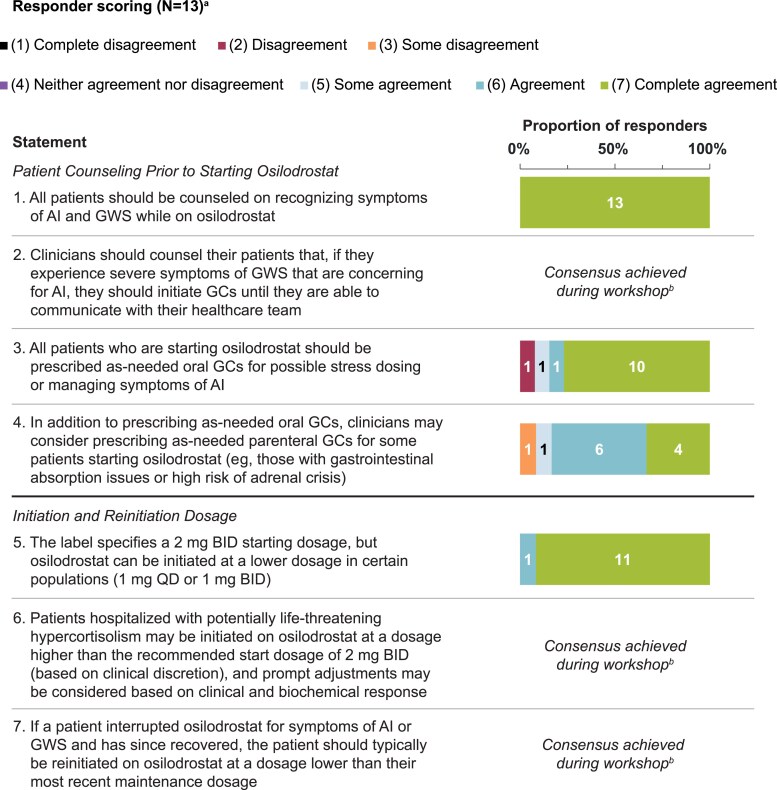
Methods: A modified Delphi consensus panel study was conducted consisting of 13 specialists from high-volume endocrinology centers with experience prescribing osilodrostat. Advisors participated in 3 consensus rounds (2 anonymous surveys, 1 virtual workshop) over approximately 10 months to provide guidance and recommendations on optimal osilodrostat use.
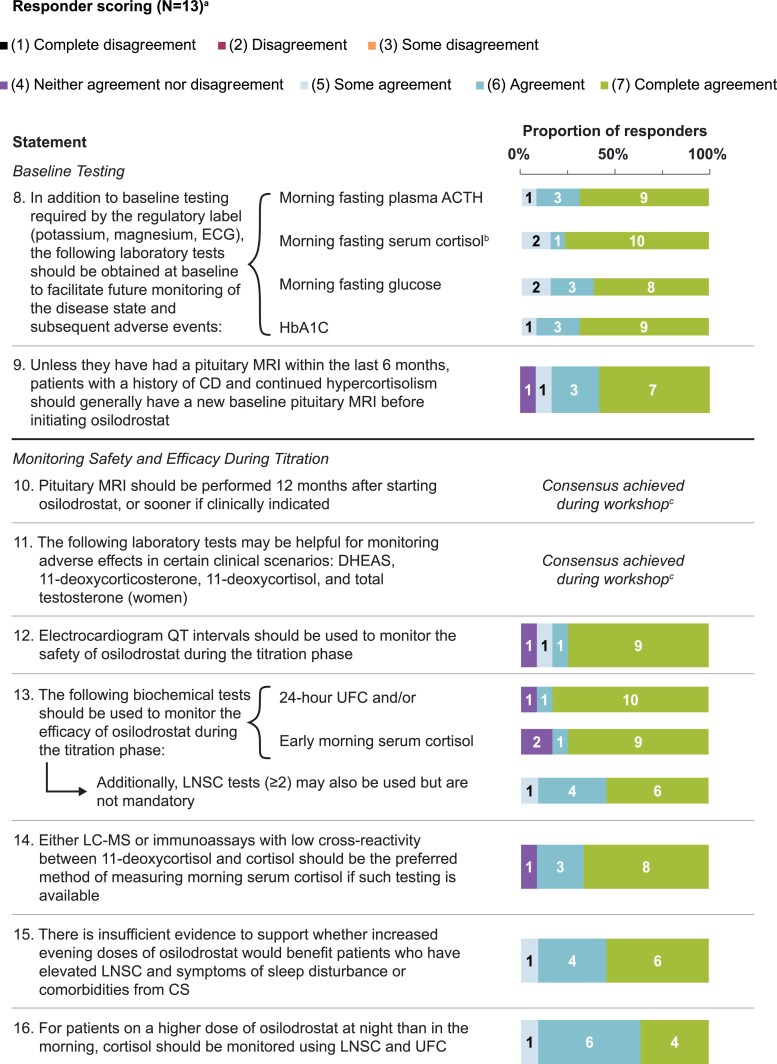
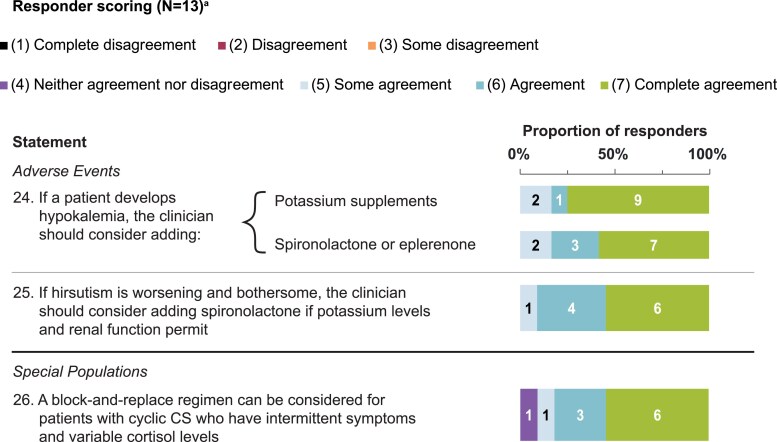
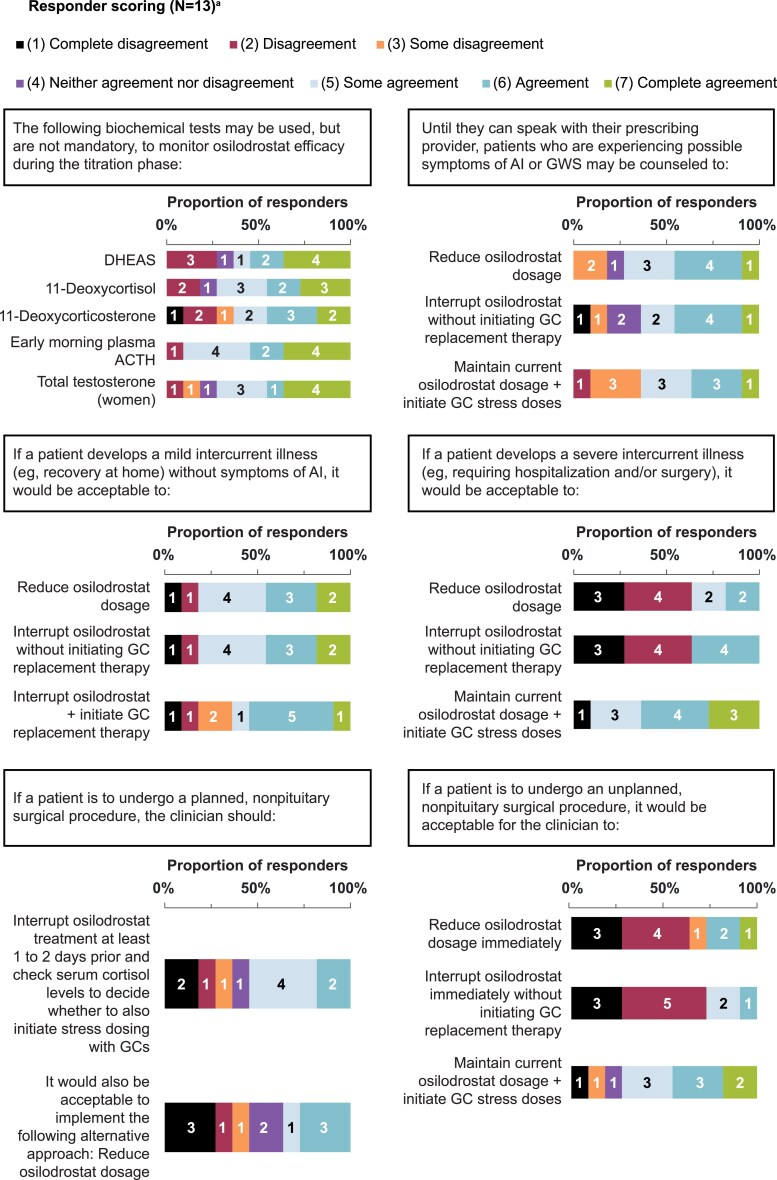
Results: Over 2 surveys and a 2-hour virtual workshop, 26 statements related to osilodrostat achieved consensus among Delphi panelists and 5 were excluded. Topics included patient preparation before osilodrostat initiation, baseline testing, dosing at onset and during treatment, managing dose adjustments, monitoring during dose titration, and treatment alterations for planned and unexpected clinical events.
Conclusion: Treatment guidance and recommendations for osilodrostat use were obtained using the Delphi method. These statements are intended to provide physicians with education and guidance on using osilodrostat to optimally treat patients with CS.
Keywords: Cushing's disease; adrenal crisis; adrenal insufficiency; endogenous Cushing's syndrome; glucocorticoid withdrawal syndrome; osilodrostat.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

References
-
- Lacroix A, Feelders RA, Stratakis CA, Nieman LK. Cushing’s syndrome. Lancet. 2015;386(9996):913‐927. - PubMed
-
- Ioachimescu AG. Prognostic factors of long-term remission after surgical treatment of Cushing’s disease. Endocrinol Metab Clin North Am. 2018;47(2):335‐347. - PubMed
-
- Findlay MC, Tenhoeve S, Alt J, et al. Predictors of durable remission after successful surgery for Cushing disease: results from the multicenter RAPID registry. Neurosurgery. 2024;95(4):761‐769. - PubMed
-
- Geer EB, Shafiq I, Gordon MB, et al. Biochemical control during long-term follow-up of 230 adult patients with Cushing disease: a multicenter retrospective study. Endocr Pract. 2017;23(8):962‐970. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources