

Switching to subcutaneous zilucoplan from intravenous complement component 5 inhibitors in generalised myasthenia gravis: a phase IIIb, open-label study
- PMID: 40620733
- PMCID: PMC12228924
- DOI: 10.1177/17562864251347283
Switching to subcutaneous zilucoplan from intravenous complement component 5 inhibitors in generalised myasthenia gravis: a phase IIIb, open-label study
Abstract
Background: Zilucoplan, a peptide complement component 5 (C5) inhibitor, is self-administered as a subcutaneous (SC) injection, which offers an alternative to intravenous infusion of antibody-based complement C5 inhibitors.
Objective: To evaluate subcutaneous zilucoplan in adults with acetylcholine receptor autoantibody-positive generalised myasthenia gravis (gMG) who switched from intravenous complement C5 inhibitors to zilucoplan.
Design: MG0017 (NCT05514873) was a phase IIIb, open-label, single-arm study.
Methods: Eligible patients had clinically stable gMG on an intravenous complement C5 inhibitor and were willing to switch to zilucoplan. Patients received a 12-week treatment period of daily subcutaneous zilucoplan 0.3 mg/kg. Incidence of treatment-emergent adverse events (TEAEs) was the primary endpoint. Change from baseline in the Myasthenia Gravis Activities of Daily Living (MG-ADL) score at Week 12 was a secondary endpoint. Treatment preference (Week 12) and treatment satisfaction (9-item Treatment Satisfaction Questionnaire for Medication (TSQM-9)) were both exploratory endpoints. Assessments by prior intravenous complement C5 inhibitor were conducted post hoc.
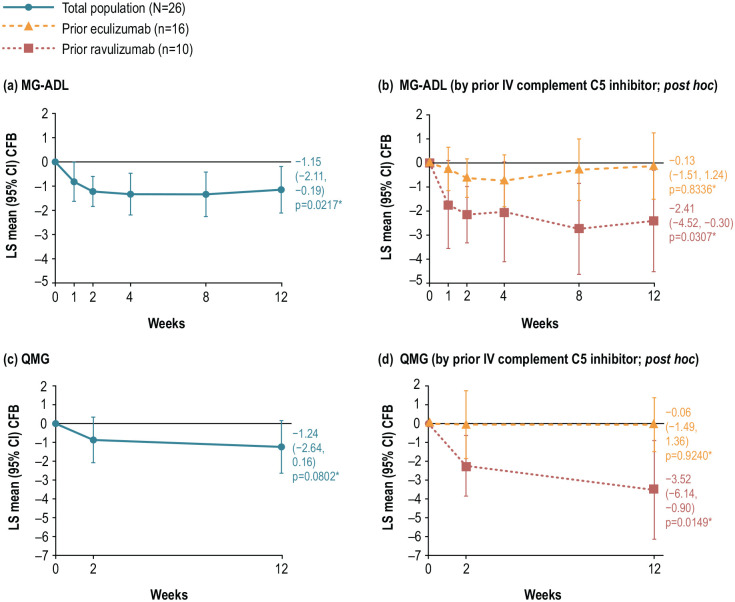
Results: Twenty-six patients enrolled and received zilucoplan; 16 switched from eculizumab and 10 from ravulizumab. TEAEs occurred in 19/26 (73.1%) patients and were mostly mild in severity. At Week 12, least squares (LS) mean (95% confidence interval) MG-ADL scores improved from baseline by -1.15 (-2.11, -0.19), p = 0.0217 and Quantitative MG (QMG) scores by -1.24 (-2.64, 0.16), p = 0.0802. Clinically meaningful improvement from baseline in mean MG-ADL and QMG scores was observed at Week 12 among patients who switched from ravulizumab (-2.41 (-4.52, -0.30; p = 0.0307) and -3.52 (-6.14, -0.90; p = 0.0149), respectively). At Week 12, 76.9% (n = 20) patients preferred subcutaneous injection compared with intravenous infusion. Mean (standard deviation) changes from baseline in the TSQM-9 Global Satisfaction, Effectiveness and Convenience subscores at Week 12 were +19.410 (27.429), +13.889 (21.534) and +21.739 (19.955), respectively. Complement inhibition increased from baseline and was complete (>95%) by Week 2 and maintained to Week 12.
Conclusion: Zilucoplan demonstrated a favourable safety profile. gMG symptoms improved during zilucoplan treatment; this was clinically meaningful for those switching from ravulizumab.
Trial registration: ClinicalTrials.gov (NCT05514873); 22 August 2022. https://clinicaltrials.gov/study/NCT05514873.
Keywords: complement inhibitor; eculizumab; myasthenia gravis; ravulizumab; zilucoplan.
Plain language summary
Experiences of patients with myasthenia gravis who switched their treatments from intravenous infusions of ravulizumab or eculizumab to self-administered daily injections of zilucoplan: effects on symptoms, safety, and patient preference Myasthenia gravis (MG) is a chronic autoimmune disease. Complement, part of the immune system, is overactive in MG. This damages the connections between muscles and nerves, causing muscle weakness. Symptoms can be reduced by blocking complement activity. Ravulizumab and eculizumab are complement inhibitors that are given as intravenous (into a vein) infusions by a healthcare professional in a hospital or clinic. Zilucoplan is another type of complement inhibitor, which patients can inject subcutaneously (under the skin) themselves. This study followed patients with MG who wanted to switch from ravulizumab or eculizumab to zilucoplan. Side effects were recorded throughout the study. Patients’ symptoms were measured to see if there was any change since switching treatment. All 26 patients who enrolled in the study had stable symptoms with their current treatment (which was ravulizumab in 10 patients, and eculizumab in 16 patients). Once enrolled, patients switched to daily zilucoplan for 12 weeks. Their main reasons for wanting to switch treatment were challenges with intravenous infusions, including travelling to hospital and long infusion times. Some patients also felt their current treatment was wearing off. After 12 weeks of zilucoplan treatment, symptoms across the group as a whole had improved. Symptoms had either improved or stayed the same in approximately 75% of patients. Symptom improvements were greatest in patients who switched from ravulizumab to zilucoplan. At the end of the study, 76.9% (20 out of 26) patients said they preferred injections with zilucoplan to intravenous infusions of their previous treatment. Side effects occurred in 73.1% of patients, which were mostly mild. Although the study was short and limited to a small number of patients, the results suggest that switching to zilucoplan is an option for patients with MG who would prefer self-injections to intravenous infusions. Longer-term studies are needed to confirm these findings.
© The Author(s), 2025.
Figures




References
-
- Gilhus NE, Verschuuren JJ. Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol 2015; 14: 1023–1036. - PubMed
-
- Gilhus NE, Tzartos S, Evoli A, et al. Myasthenia gravis. Nat Rev Dis Primers 2019; 5: 30. - PubMed
-
- Howard JF, Jr, Vissing J, Gilhus NE, et al. Zilucoplan: an investigational complement C5 inhibitor for the treatment of acetylcholine receptor autoantibody-positive generalized myasthenia gravis. Expert Opin Investig Drugs 2021; 30: 483–493. - PubMed
-
- Howard JF, Jr, Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol 2017; 16: 976–986. - PubMed
-
- Howard JF, Jr, Bresch S, Genge A, et al. Safety and efficacy of zilucoplan in patients with generalised myasthenia gravis (RAISE): a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Neurol 2023; 22: 395–406. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
