

A Quiet Rupture: Hemodynamically Stable Ruptured Descending Thoracic Aortic Aneurysm Presenting as Lower Respiratory Tract Infection
- PMID: 40621330
- PMCID: PMC12227835
- DOI: 10.7759/cureus.85375
A Quiet Rupture: Hemodynamically Stable Ruptured Descending Thoracic Aortic Aneurysm Presenting as Lower Respiratory Tract Infection
Abstract
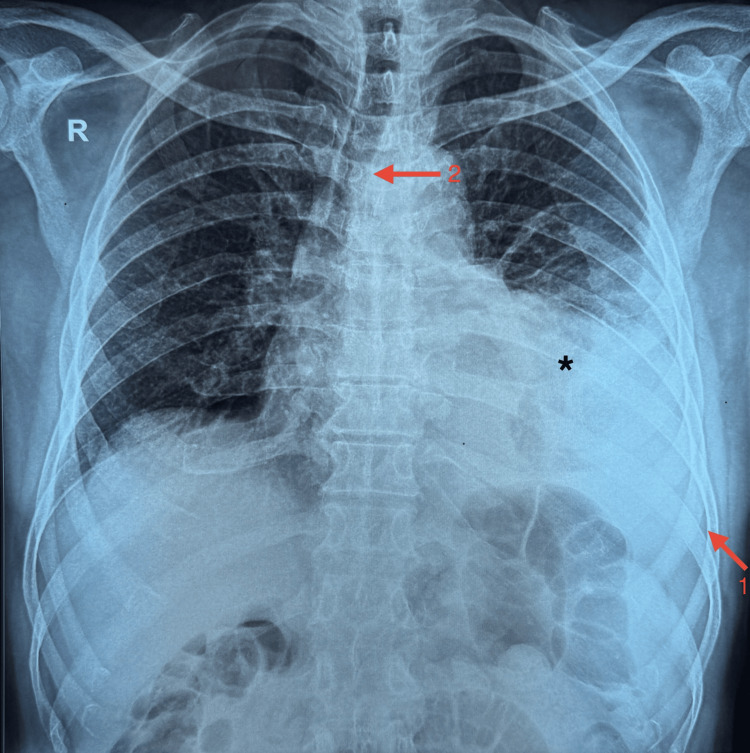
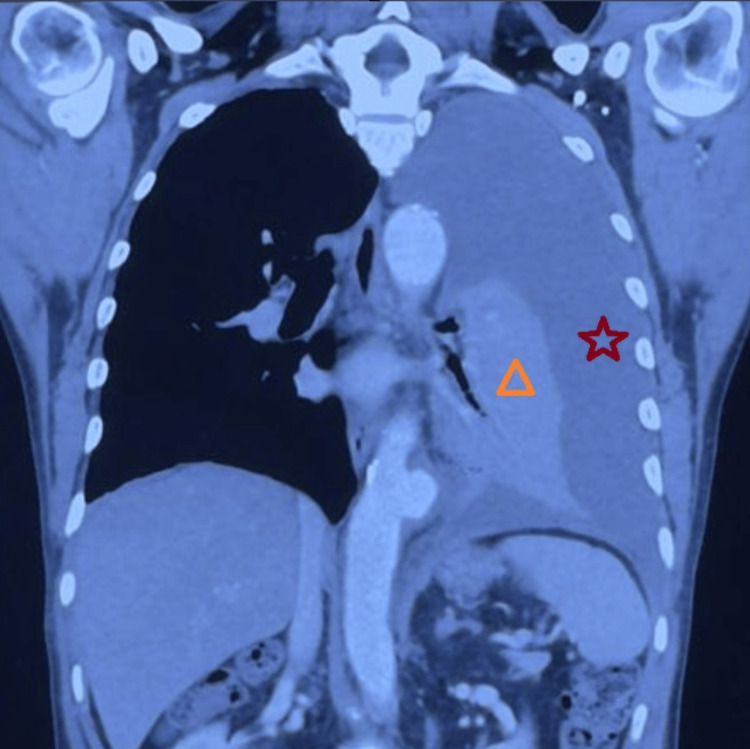
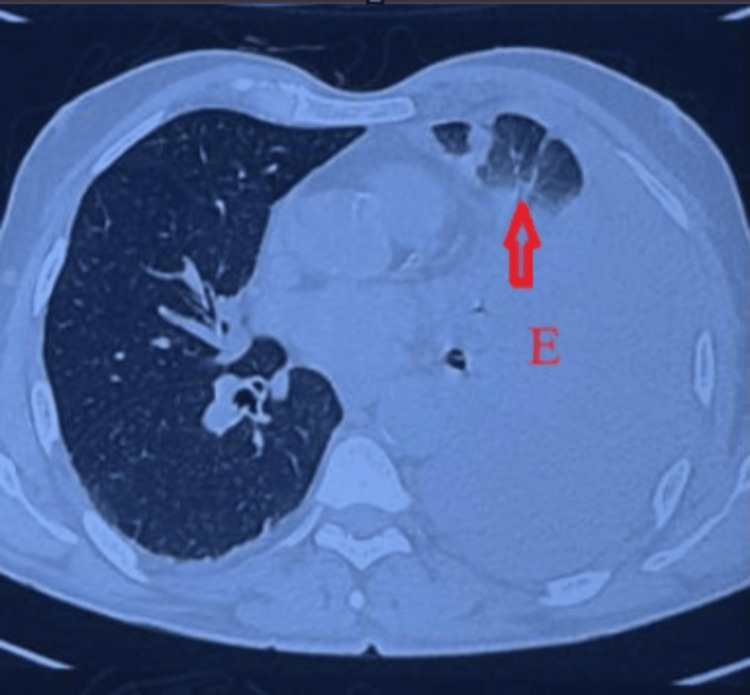
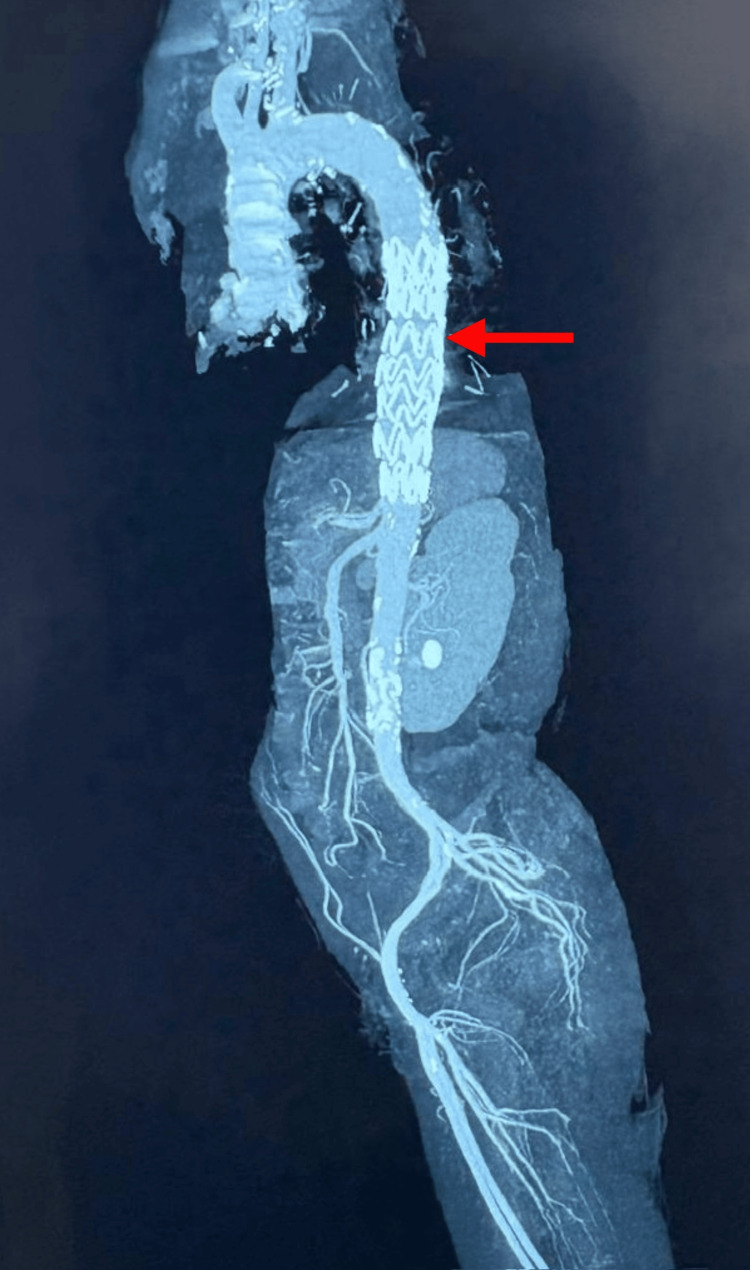
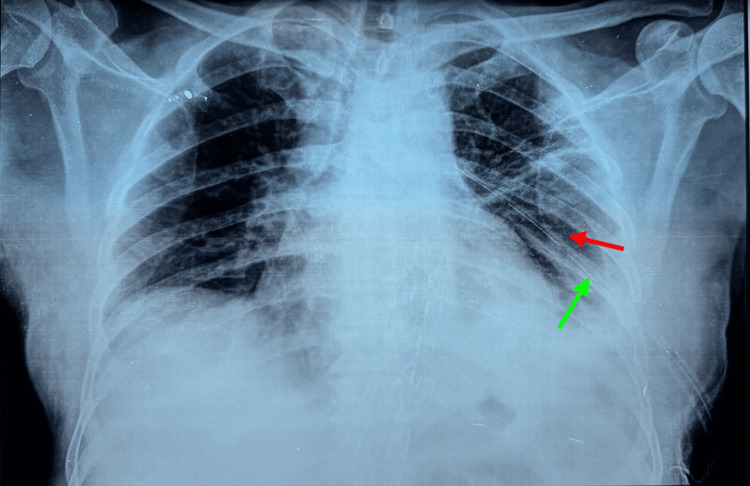
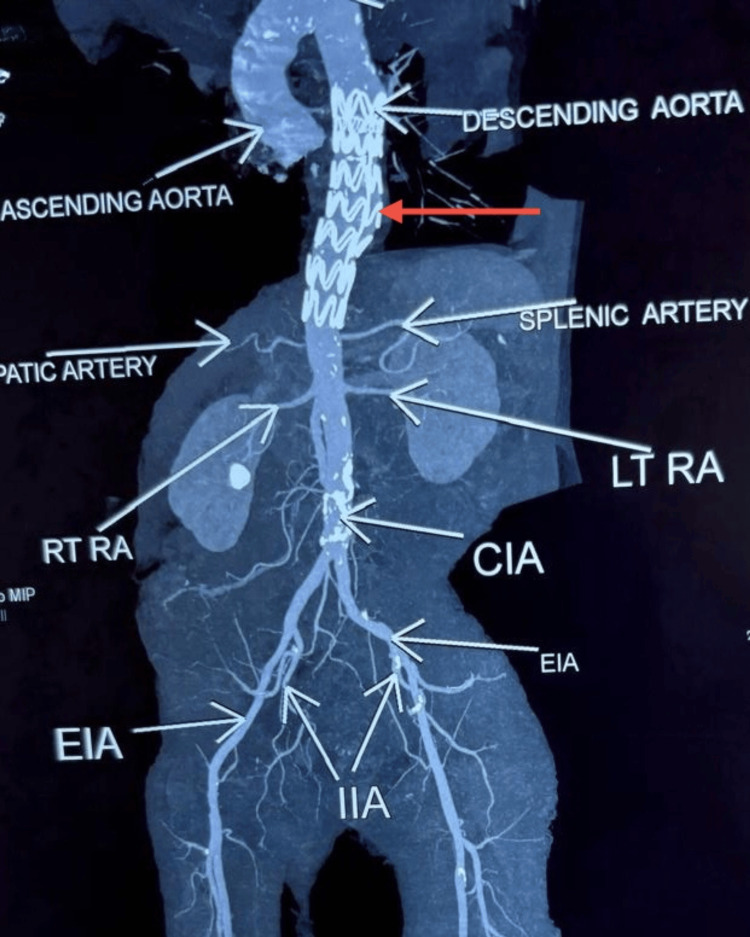
The rupture of a descending thoracic aortic aneurysm (DTAA) is a rare but critical vascular emergency that requires immediate recognition and action. It usually presents as a sharp, severe pain in the chest or back; however, some individuals exhibit non-typical symptoms resembling respiratory infections, leading to misdiagnosis and delays in definitive treatment. A 63-year-old male with a history of hypertension and smoking presented with left-sided chest pain to another hospital, where he was diagnosed with unstable angina based on clinical suspicion and managed conservatively with anti-anginal medication. Over the next three days, the patient developed a persistent cough, low-grade fever, and pleuritic pain, prompting referral to our hospital, where a lower respiratory tract infection (LRTI) was considered. On arrival, he was hemodynamically stable with a systolic BP of 100 mmHg and was managed with intravenous fluids, antibiotics, and nebulizers. Chest X-ray revealed moderate left pleural effusion with tracheal deviation, and thoracic ultrasound confirmed internal echoes suggestive of hemorrhagic content. Diagnostic thoracentesis yielded hemorrhagic fluid, prompting high-resolution computed tomography (HRCT), which showed a partially thrombosed 54 mm × 49 mm saccular aneurysm of the descending thoracic aorta with left lung collapse. Despite the rupture, the patient remained hemodynamically stable, suggestive of a contained event. A subsequent computed tomography angiogram (CTA) confirmed rupture into the pleural space and was the imaging modality that established the final diagnosis. The patient underwent thoracic endovascular aortic repair (TEVAR) using a 30 mm × 30 mm × 120 mm Ankura graft, selected for its conformability and effective sealing profile in emergencies. Postoperative recovery was uneventful. A CT aortogram on day three confirmed complete exclusion of the aneurysm with no endoleak, and a follow-up chest X-ray at two weeks showed full resolution of the hemothorax. This case illustrates the diagnostic challenge posed by atypical ruptured DTAA presentations and reinforces the importance of early CTA in unexplained pleural effusions, even in stable patients. Structured post-TEVAR surveillance remains critical to ensure long-term outcomes.
Keywords: aortic emergency; contained aortic rupture; ct angiography; descending thoracic aortic aneurysm; diagnostic delay; hemothorax; high-resolution ct; lower respiratory tract infection mimic; misdiagnosis; tevar.
Copyright © 2025, N.K. et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Endovascular treatment for ruptured abdominal aortic aneurysm.Cochrane Database Syst Rev. 2017 May 26;5(5):CD005261. doi: 10.1002/14651858.CD005261.pub4. Cochrane Database Syst Rev. 2017. PMID: 28548204 Free PMC article.
-
Aorto-Right Atrial Fistula Caused by Subacute Type A Aortic Dissection Six Months After Double Valve Replacement: A Case Report and Literature Review.Cureus. 2025 Jun 24;17(6):e86692. doi: 10.7759/cureus.86692. eCollection 2025 Jun. Cureus. 2025. PMID: 40718171 Free PMC article.
-
Laparoscopic surgery for elective abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 May 4;5(5):CD012302. doi: 10.1002/14651858.CD012302.pub2. Cochrane Database Syst Rev. 2017. PMID: 28471523 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Ultrasonography for endoleak detection after endoluminal abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 Jun 9;6(6):CD010296. doi: 10.1002/14651858.CD010296.pub2. Cochrane Database Syst Rev. 2017. PMID: 28598495 Free PMC article.
References
-
- Ruptured thoracic aortic aneurysms: a study of incidence and mortality rates. Johansson G, Markström U, Swedenborg J. J Vasc Surg. 1995;21:985–988. - PubMed
-
- Unusual cause of hemorrhagic pleural effusion: a case report. Lee KT, Leong KN, Chow TS, Wong PS. World J Clin Infect Dis. 2022;12:41–46.
Publication types
LinkOut - more resources
Full Text Sources