

Immunotherapy in metastatic prostate cancer
- PMID: 40621483
- PMCID: PMC12227887
- DOI: 10.1177/17588359251347857
Immunotherapy in metastatic prostate cancer
Abstract
Over the last 15 years, immunotherapy has revolutionised treatment paradigms and improved outcomes in a range of malignancies. Despite these advances, the role of immunotherapy in standard prostate cancer (PCa) management is limited, and Sipuleucel-T is the only approved immunotherapeutic agent. This article reviews the role of checkpoint inhibitors (ICIs), T-cell engagers (TCEs) and chimeric antigen receptor (CAR)-T cells in PCa treatment. Phase II/III trials of ICIs as monotherapy or combination treatment have been negative to date. Early phase data for TCE are promising, but the feasibility of adoption of TCEs into the clinic will depend on overcoming neutralising anti-drug antibodies and limiting toxicities. CAR-T cells have demonstrated feasibility and acceptable safety profiles in early phase clinical trials, and it is hoped that the ongoing development of later-generation constructs and therapeutic combinations will enhance outcomes.
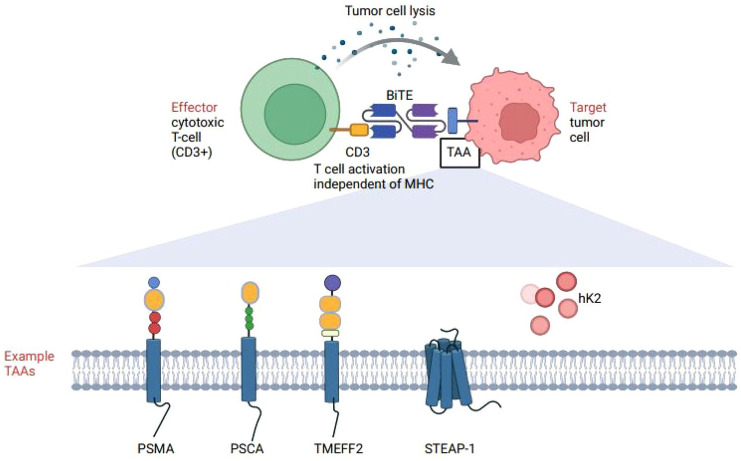
Keywords: BiTE; CAR-T cell; T cell engager therapy; bispecific T cell engager; checkpoint inhibitor; chimeric antigen receptor-T cell; immunotherapy; prostate cancer.
Plain language summary
The current and future role of immunotherapy in prostate cancer Over the past 15 years, traditional forms of immunotherapy have revolutionised survival from some ‘hot’ cancers, such as melanoma and other skin cancers. Immune cell ‘cold’ cancers, such as prostate cancer, are resistant to traditional immunotherapy. Here, we explain some of the reasons behind the failure of traditional immunotherapy in prostate cancer. We also review new types of immunotherapy which look promising as ways to overcome resistance and harness the immune system against prostate cancer cells. We suggest that newer forms of immunotherapy are worthy of ongoing development in the treatment of prostate cancer.
© The Author(s), 2025.
Conflict of interest statement
Liam Dwyer declares no potential conflicts of interest with respect to the research, authorship and/or publication of this article. Claudia Leslie declares no potential conflicts of interest with respect to the research, authorship and/or publication of this article. Rhiannon Mellor declares no potential conflicts of interest with respect to the research, authorship and/or publication of this article. Renea A. Taylor has research collaborations with Pfizer, Astellas, Zenith Epigenetics and AstraZeneca. Lisa Horvath: Site investigator on PRINCE, KEYNOTE-991, Checkmate 9KD, COSMIC021, NCT03792841 (AMG160), NCT04221542 (phase 1 AMG509), NCT06691984 (AMG509 phase III). Received research funding from Bayer and RedHill Biopharma (through ANZUP) and Astellas (through COBLH institution). Received travel and honoraria (all through COBLH institution) from Bayer, Astellas, Janssen, MSD and Pfizer. Advisory boards for Amgen, Astellas, Bayer and Janssen. Tahlia Scheinberg received research funding from Bayer (paid to ANZUP) and conference travel support from Bayer. She is a named inventor for a patent (PCT/AU2023/050849).
Figures


References
-
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024; 74(3): 229–263. - PubMed
-
- Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 2017; 377(4): 352–360. - PubMed
-
- Chi K, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med 2019; 381(1): 13–24. - PubMed
-
- Davis I, Martin A, Stockler M, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med 2019; 381(2): 121–131. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
