

Long-Gap Sciatic Nerve Regeneration Using 3D-Printed Nerve Conduits with Controlled FGF-2 Release
- PMID: 40621679
- PMCID: PMC12278209
- DOI: 10.1021/acsami.5c08237
Long-Gap Sciatic Nerve Regeneration Using 3D-Printed Nerve Conduits with Controlled FGF-2 Release
Abstract
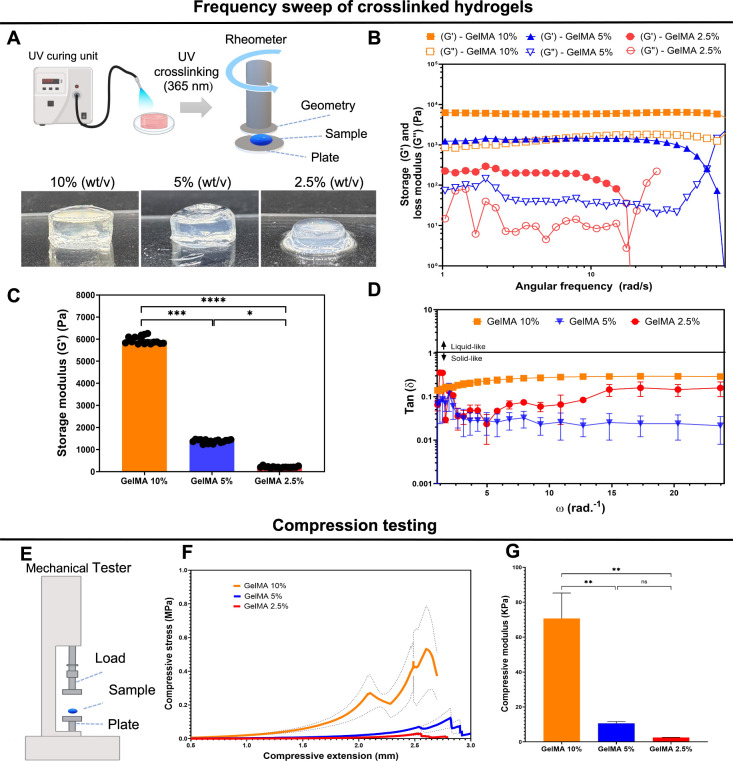
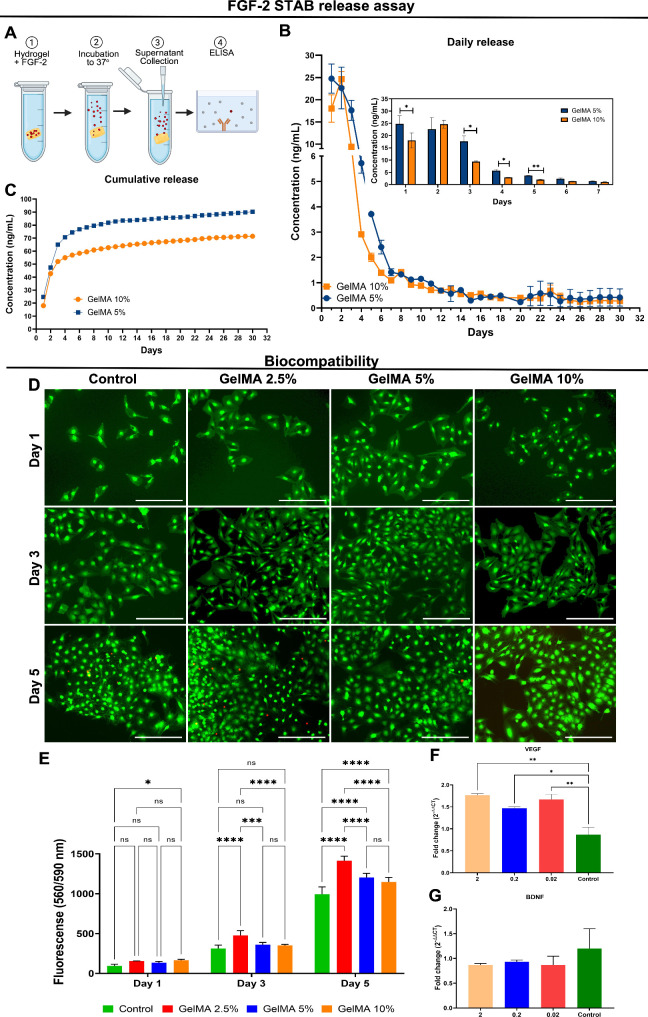
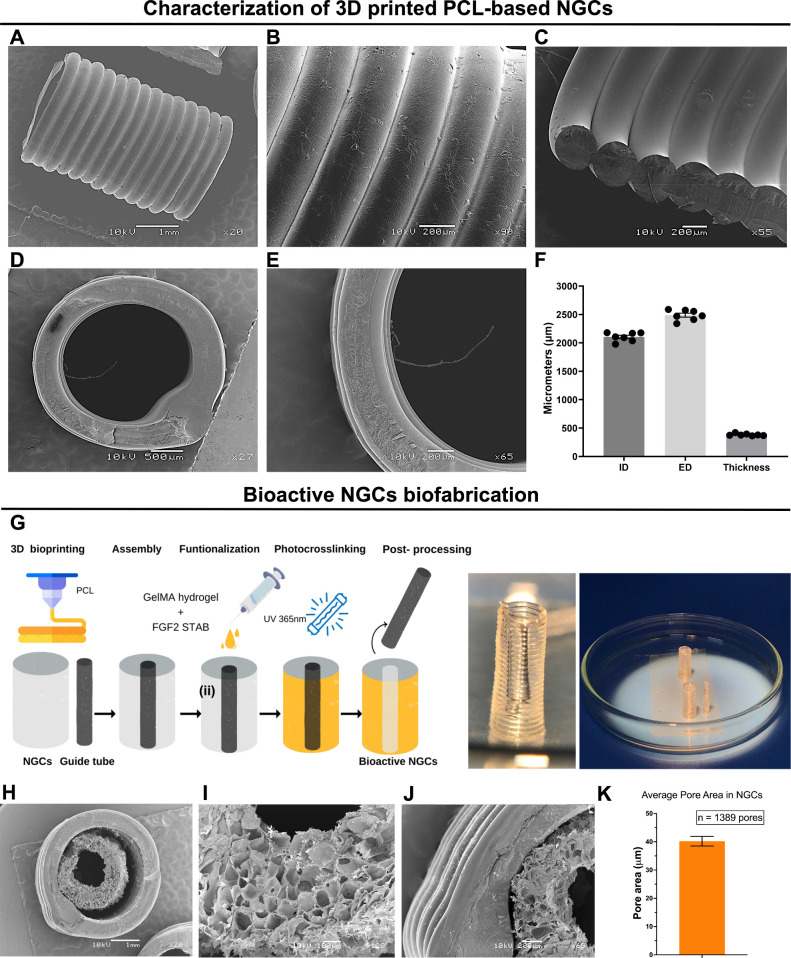
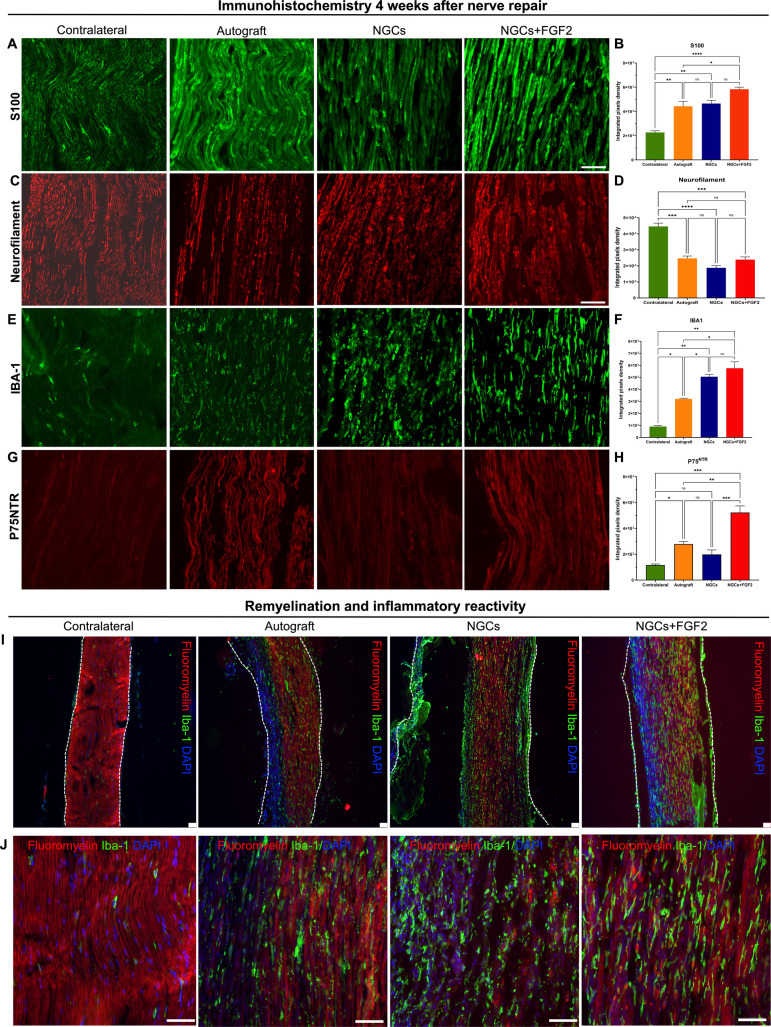
Peripheral nerve injuries (PNIs) by transection require reconstructive surgery, often with highly variable results and persistent sensory and motor deficits. Three-dimensional (3D) printing enables the biofabrication of nerve guidance conduits (NGCs) with the ability to release neurotrophic factors, showing therapeutic potential. We developed a 3D printing process of NGCs using polycaprolactone (PCL) and gelatin methacryloyl (GelMA) integrated with a thermostable fibroblast growth factor 2 (FGF-2). The synthesized GelMA at 10% (w/v) concentration showed superior rheological, mechanical, and ultrastructural characteristics, ensuring 3D printing fidelity. Incorporating FGF-2 into GelMA resulted in a controlled release pattern over 30 days along with biocompatibility and an increase of metabolism in rat S16 Schwann cells and human mesenchymal stem cells (MSCs). MSCs exhibited gene regulation linked to vascularization after FGF-2 stimulation. The PCL polymer facilitated the buildability of a spiral-patterned tubular structure, which was functionalized with a combination of GelMA and UV photocrosslinked. At 12 weeks, following a long-gap nerve injury in rats, NGC implantation enhanced sensory and motor recovery, improved electrophysiological function, and promoted morphological and ultrastructural nerve reorganization and regeneration. At 4 weeks, significant Schwann cell proliferation (S100), expression of the pan-neurotrophin receptor (P75NTR), myelination of newly grown axons, and organization of neurofilaments were observed. The bioactive NGCs represent a promising alternative to nerve autografts for the repair of long-gap injuries.
Keywords: 3D printing; FGF-2; biomaterials; gelatin methacryloyl; nerve guidance conduits; peripheral nerve regeneration; polycaprolactone.
Figures





References
-
- Huckhagel T., Nüchtern J., Regelsberger J., Lefering R.. Nerve Injury in Severe Trauma with Upper Extremity Involvement: Evaluation of 49,382 Patients from the TraumaRegister DGU® between 2002 and 2015. Scand. J. Trauma. Resusc. Emerg. Med. 2018;26(1):76. doi: 10.1186/s13049-018-0546-6. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
