

External validation of a prediction model for disability and pain after lumbar disc herniation surgery: a prospective international registry-based cohort study
- PMID: 40622239
- PMCID: PMC12232440
- DOI: 10.2340/17453674.2025.44251
External validation of a prediction model for disability and pain after lumbar disc herniation surgery: a prospective international registry-based cohort study
Abstract
Background and purpose: We aimed to externally validate machine learning models developed in Norway by evaluating their predictive outcome of disability and pain 12 months after lumbar disc herniation surgery in a Swedish and Danish cohort.
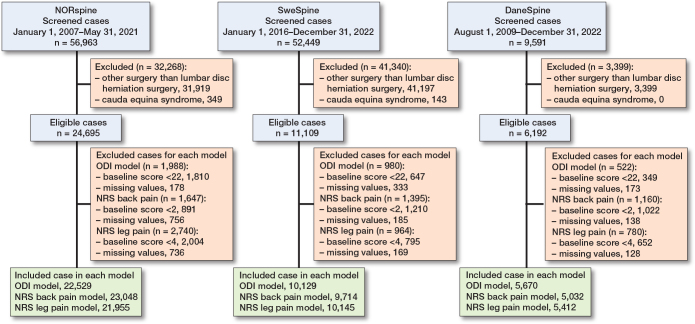
Methods: Data was extracted for patients undergoing microdiscectomy or open discectomy for lumbar disc herniation in the NORspine, SweSpine and DaneSpine national registries. Outcome of interest was changes in Oswestry disability index (ODI) (≥ 22 points), Numeric Rating Scale (NRS) for back pain (≥ 2 points), and NRS for leg pain (≥ 4 points). Model performance was evaluated by discrimination (C-statistic), calibration, overall fit, and net benefit.
Results: For the ODI model, the NORspine cohort included 22,529 patients, the SweSpine cohort included 10,129 patients, and DaneSpine 5,670 patients. The ODI model's C-statistic varied between 0.76 and 0.81 and calibration slope point estimates varied between 0.84 and 0.99. The C-statistic for NRS back pain varied between 0.70 and 0.76, and calibration slopes varied between 0.79 and 1.03. The C-statistic for NRS leg pain varied between 0.71 and 0.74, and calibration slopes varied between 0.90 and 1.02. There was acceptable overall fit and calibration metrics with minor-modest but explainable heterogeneity observed in the calibration plots. Decision curve analyses displayed clear potential net benefit in treatment in accordance with the prediction models compared with treating all patients or none.
Conclusion: Predictive performance of machine learning models for treatment success/non-success in disability and pain at 12 months post-surgery for lumbar disc herniation showed acceptable discrimination ability, calibration, overall fit, and net benefit reproducible in similar international contexts. Future clinical impact studies are required.
Figures


References
-
- Lagerbäck T, Fritzell P, Hägg O, Nordvall D, Lønne G, Solberg T K, et al. Effectiveness of surgery for sciatica with disc herniation is not substantially affected by differences in surgical incidences among three countries: results from the Danish, Swedish and Norwegian spine registries. Eur Spine J 2019; 28(11): 2562-71. doi: 10.1007/s00586-018-5768-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
