

Exogenous Hormones, Tumor Intrinsic Subtypes, and Breast Cancer
- PMID: 40622713
- PMCID: PMC12235495
- DOI: 10.1001/jamanetworkopen.2025.19236
Exogenous Hormones, Tumor Intrinsic Subtypes, and Breast Cancer
Abstract
Importance: Etiologic heterogeneity in breast carcinogenesis needs to be well characterized for targeted prevention. Associations between menopausal hormonal therapy (MHT) and oral contraceptive (OC) use and breast cancer intrinsic-like subtypes are not well understood.
Objective: To examine whether exogenous hormone use is differentially associated with breast cancer subtypes and to evaluate heterogeneity by intrinsic-like subtypes.
Design, setting, and participants: This study pooled data from 31 nested and population-based case-control studies involved in the Breast Cancer Association Consortium. The study population included individuals with breast cancer and control participants from 13 case-control studies nested in prospective cohorts (recruited between 1982 and 2011) and 18 population-based case-control studies (recruited between 1990 and 2013). Data analysis was performed in June 2024.
Exposure: MHT use (estrogen-progestin therapy [EPT] or estrogen-only therapy [ET]) in postmenopausal women and OC use in premenopausal women (never, past use, or current use).
Main outcomes and measures: Breast cancer intrinsic-like subtypes (luminal A-like, luminal B-like, luminal B-ERBB2 [formerly HER2 or HER2/neu]-like, ERBB2 enriched-like, or triple-negative) were determined by immunohistochemistry of tumor sections. Polytomous logistic regression was performed to estimate the association between exogenous hormones and risk of breast cancer by intrinsic-like subtypes. Analyses by subtypes were stratified by body mass index (BMI [calculated as weight in kilograms divided by height in meters squared]; healthy weight, 18.5-<25; overweight, 25-<30; or obesity, ≥30).
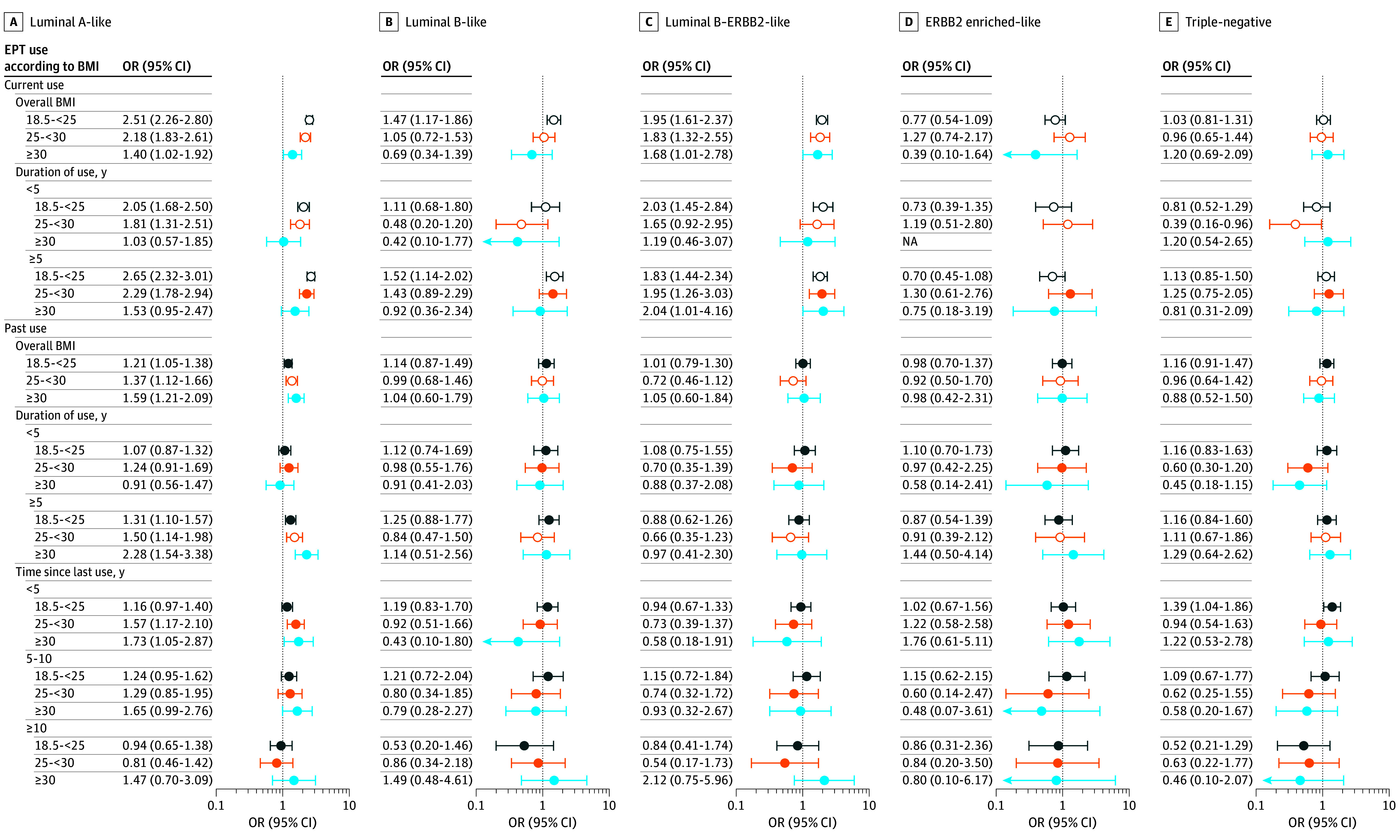
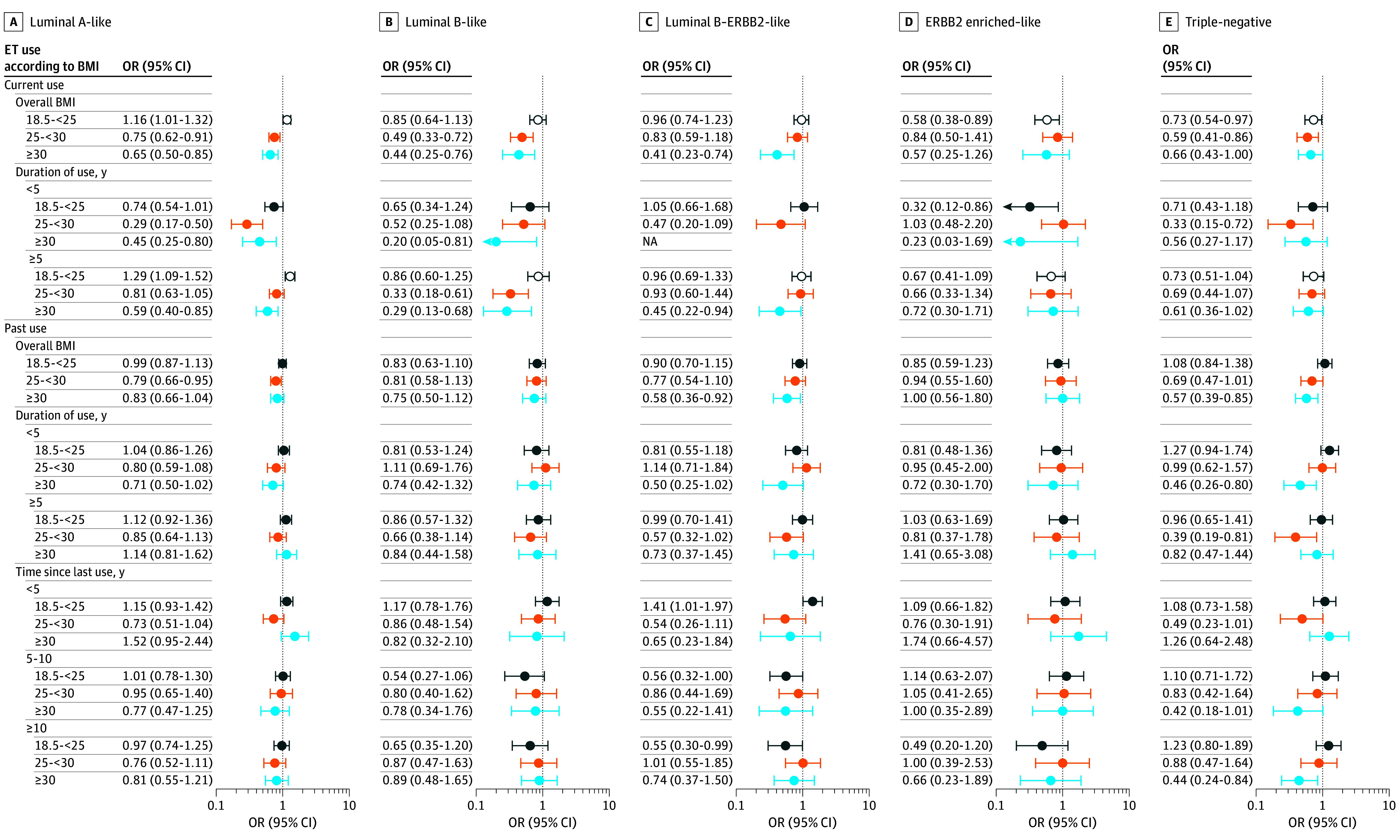
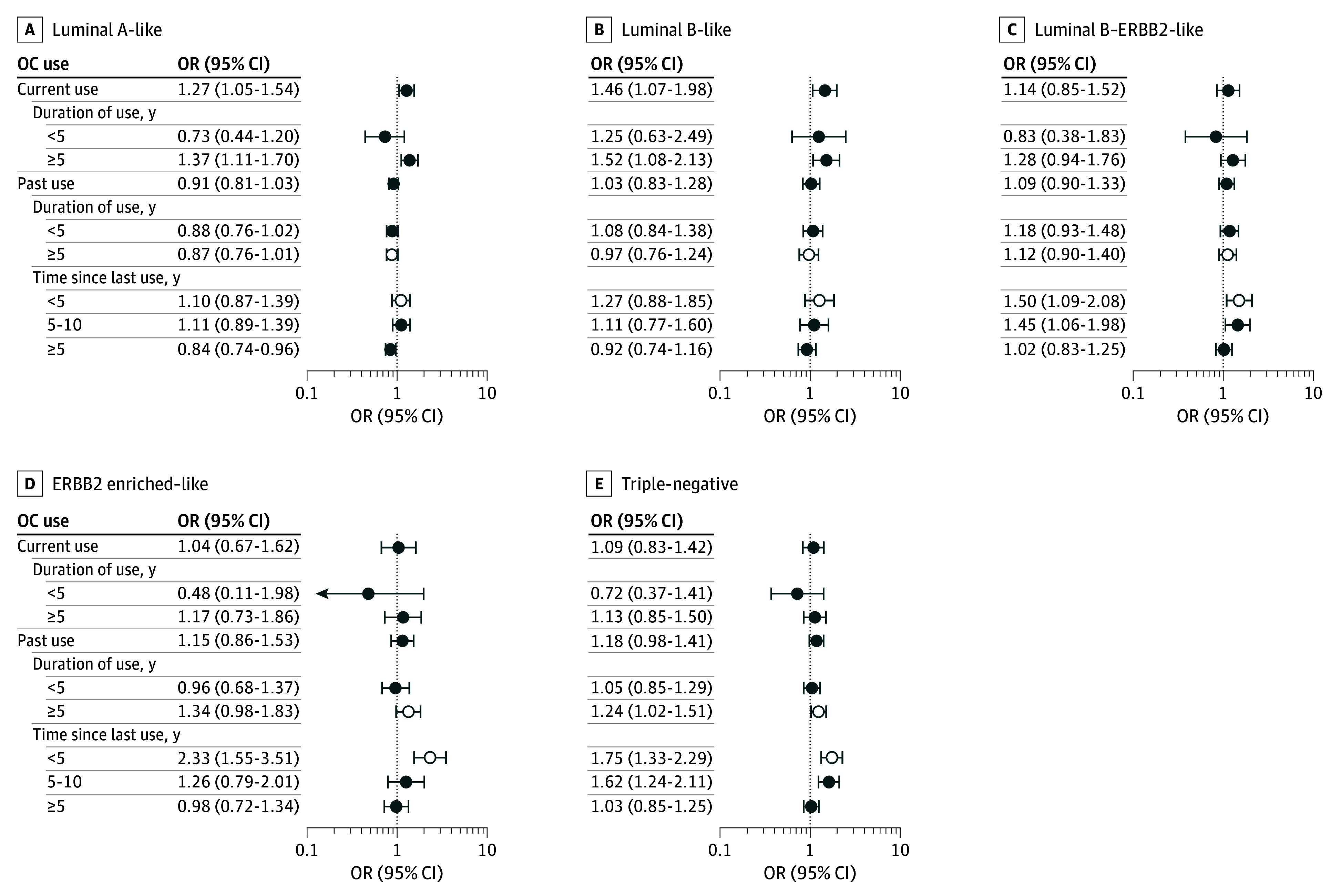
Results: This study included 42 269 individuals with breast cancer (11 901 [28.2%] premenopausal and 30 368 [71.8%] postmenopausal; 23 353 [55.2%] had a known intrinsic-like subtype) and 71 072 control participants. The mean (SD) age of all participants was 57.9 (10.9) years. In postmenopausal women, associations between current MHT use (EPT or ET) and breast cancer differed by subtype. Current EPT users with healthy weight were more likely to be diagnosed with luminal A-like (odds ratio [OR], 2.51 [95% CI, 2.26-2.80]) or luminal B-ERBB2-like (OR, 1.95 [95% CI, 1.61-2.37]) subtypes. These associations were attenuated but remained for individuals with overweight (OR, 1.40 [95% CI, 1.02-1.92]) or obesity (OR, 1.68 [95% CI, 1.01-2.78]). EPT use increased the odds of being diagnosed with luminal B-like tumors solely in women with healthy weight (OR, 1.47 [95% CI, 1.17-1.86]). Current ET use was positively associated with luminal A-like disease in women with healthy weight only (OR, 1.16 [95% CI, 1.01-1.32]), showing inverse associations with higher BMI (obesity: OR, 0.65 [95% CI, 0.50-0.85]). In premenopausal women, recent OC use was associated with luminal B-ERBB2-like (OR, 1.50 [95% CI, 1.09-2.08]), ERBB2 enriched-like (OR, 2.33 [95% CI, 1.55-3.51]), and triple-negative (OR, 1.75 [95% CI, 1.33-2.29]; P < .04 for heterogeneity) tumors.
Conclusions and relevance: In this study, clear differences were observed in associations between current EPT use and luminal-like breast cancer subtypes and other subtypes. EPT users with healthy weight were more likely to be diagnosed with luminal-like breast cancer compared with nonusers. Subtype heterogeneity was less apparent in associations of OC and ET use. Future studies on contemporary formulations, patterns of use, and routes of administration of exogenous hormone usage are warranted.
Conflict of interest statement
Figures
References
-
- Wang K, Li F, Chen L, Lai YM, Zhang X, Li HY. Change in risk of breast cancer after receiving hormone replacement therapy by considering effect-modifiers: a systematic review and dose-response meta-analysis of prospective studies. Oncotarget. 2017;8(46):81109-81124. doi: 10.18632/oncotarget.20154 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
