

Epidemiological characteristics and management of Gram-negative bacteraemia in different immunocompromised hosts: Observational single-center study
- PMID: 40622988
- PMCID: PMC12233224
- DOI: 10.1371/journal.pone.0327535
Epidemiological characteristics and management of Gram-negative bacteraemia in different immunocompromised hosts: Observational single-center study
Abstract
Importance: Patients with Gram-negative bloodstream infections (GN-BSI) are classified as non-immunocompromised (n-IC) or immunocompromised (IC). However, immunosuppressive condition should not be considered univocally.
Objective: To investigate epidemiological characteristics, management and outcome of GN-BSI in IC and non-IC patients.
Methods: Retrospective single-center study of hospitalized patients with GN-BSI conducted over a 7-year period. Patients with GN-BSI were divided in: solid organ transplant (SOT) recipients, patients with hematologic malignancy (HM), patients with metastatic solid cancer (mSC), and non-major IC patients (nm-IC).
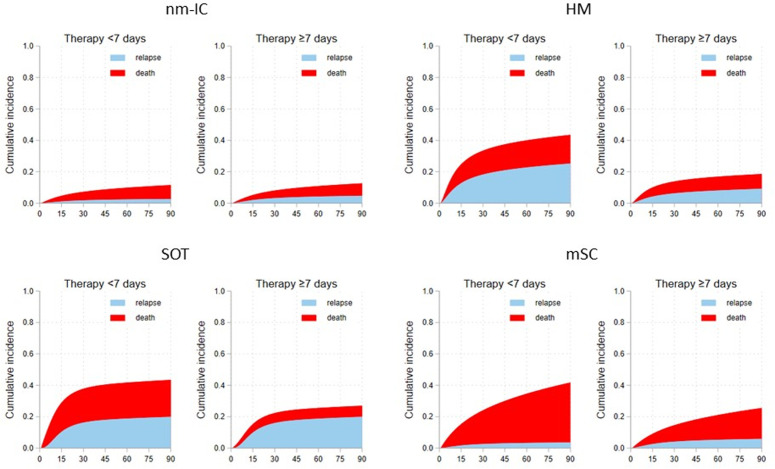
Results: 3544 patients analysed: 76.7% nm-IC, 6.5% SOT, 8.0% HM and 8.8% mSC. SOT and HM patients were younger (SOT: 56.6 ± 13.1 years; HM: 56.4 ± 14.5; nm-IC: 72.4 ± 16.1; mSC: 68.6 ± 13.1, p < 0.001) and had lower CCI value (SOT: 4.5 ± 2.4; HM: 4.1 ± 2.1; nm-IC: 5.5 ± 2.6; mSC: 9.7 ± 2.5, p < 0.001). Urinary tract infection was the most common source of BSI in nm-IC (nm-IC: 50.1%, HM:15%; SOT: 33.3%; mSC: 25.9%, p < 0.001), intra-abdominal infection was the more frequent source among SOT and mSC (SOT:42.3%; mSC: 49.3%, nm-IC: 27.8%, HM:29%; p < 0.001). Primary BSI was the first cause of GN-BSI in HM (HM: 62.1%; SOT: 18.5%; nm-IC: 17.2%; mSC: 10.6%, p < 0.001). The lowest rate of death was observed in SOT and the highest in mSC (SOT 8.2%; nm-IC 13.4%; HM 14.9%; mSC 19.9%, p < 0.001). Relapse rate was highest in SOT (SOT: 18.8%; HM: 11.8%; NMIC: 7.2%; aST: 7.1%, p < 0.001). Follow-up bloodcultures were associated with a lower mortality only among NMIC (HR = 0.317, 95% CI 0.178-0.563, p < 0.001) and aST (HR = 0.198, 95% CI 0.058-0.673, p = 0.010). The role of treatment duration on relapse was not evident in any group, conversely receiving at least 7 days of treatment was associated with a lower risk of 90-day mortality in SOT and HM patients.
Conclusions: The characteristics and outcome of GN-BSI are peculiar between specific IC categories, therefore a personalized management should be implemented.
Copyright: © 2025 Toschi et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
