

Multistage correction of severe kyphoscoliosis and pulmonary compromise in adults through combined halo-pelvic traction and posterior spinal techniques
- PMID: 40624102
- PMCID: PMC12234860
- DOI: 10.1038/s41598-025-10307-4
Multistage correction of severe kyphoscoliosis and pulmonary compromise in adults through combined halo-pelvic traction and posterior spinal techniques
Abstract
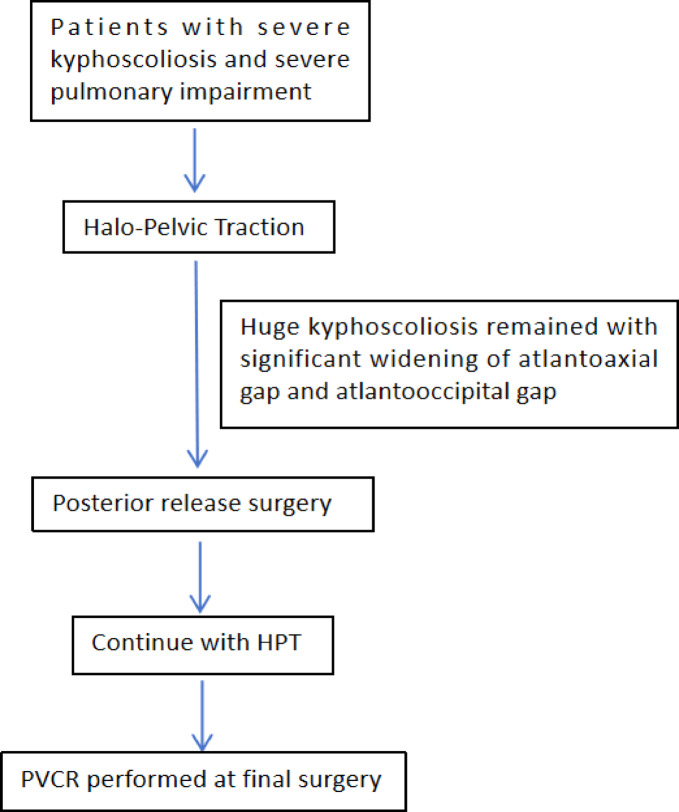
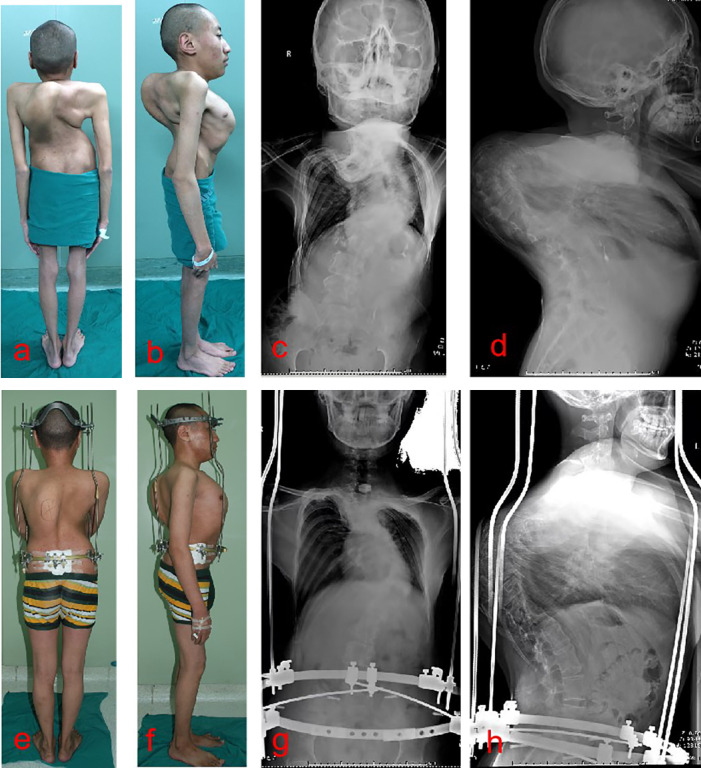
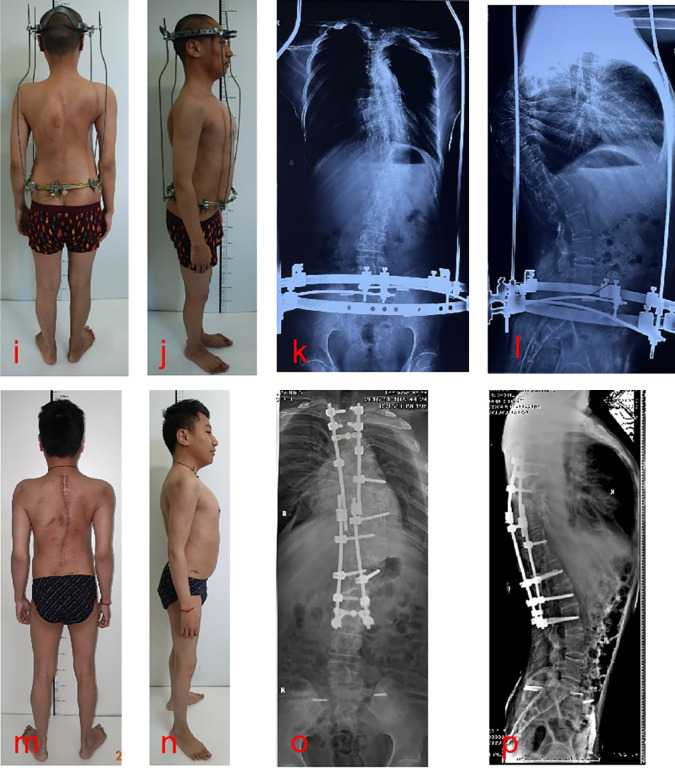
Patients with kyphoscoliosis can present with a variety of chief complaints, including axial back pain, concerns about cosmesis, progressively worsening respiratory function, and even neurological deficits. Correction of severe adult kyphoscoliosis remains challenging due to the severity of the deformity and poor cardiopulmonary function. Direct one-stage corrective surgery can lead to enormous complications and unsatisfactory outcomes when dealing with patients with severe kyphoscoliosis. Preoperative halo-pelvic traction (HPT) has become popular in the management of severe scoliosis. The present study aimed to summarize the efficacy and safety of the staged strategy. Patients with severe kyphoscoliosis complicated by severe pulmonary impairment who underwent staged treatment and met the inclusion and exclusion criteria from Jan 2019 to Jan 2020 were retrospectively reviewed. Data including patient demographics, major coronal curve and kyphosis, pulmonary function test results, distraction time, and complications at different stages of treatment were recorded. Twenty-three patients (16 male and 7 female) with severe kyphoscoliosis and severe pulmonary impairment were included in the study. The mean age of these patients was 26.2 ± 5.7 years. The mean duration of traction before posterior release surgery was 4.0 ± 1.0 months and 4.4 ± 1.0 months after posterior release surgery. Mean follow-up was 40.4 ± 3.9 months. The main curve and kyphosis at admission were 145 ± 11.8° and 149 ± 21.7°, respectively. After HPT, the main curve and kyphosis decreased to 114 ± 12.3° and 124 ± 22.9°, respectively. The FVC and FVC% at admission were 1.44 ± 0.63 L and 39.0 ± 16.19%, respectively. The FVC and FVC% improved significantly after HPT. According to the Nash-Moe classification, the rotation of the apical vertebrae was grade IV in all patients, and the rotation did not improve during the traction. The operative time for posterior release was 266 ± 49 min. The average bleeding of posterior release was 600 ± 242 ml. HPT was maintained after the posterior release surgery. The mean operating time of the posterior correction surgery was 588 ± 53 min, and the mean bleeding was 1605 ± 313 ml. Correction rates were 56.6% and 68.5% in the coronal and sagittal planes, respectively. Staged treatment is an effective and safe strategy to correct severe kyphoscoliosis complicated by severe pulmonary impairment. Preoperative HPT combined with posterior release surgery can significantly reduce spinal deformity and improve pulmonary function. Posterior vertebra column resection (PVCR) is an effective technique for correcting kyphoscoliosis, but it is a technically demanding procedure.
Keywords: Halo-pelvic traction; Posterior release surgery; Posterior vertebra column resection; Severe kyphoscoliosis; Staged treatment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: The study protocol was approved by the ethics committee of the Third People’s Hospital of Chengdu (IRB approval number: 2022-S-23). All methods were conducted in compliance with relevant guidelines, regulations, and the Declaration of Helsinki. Consent for publication: Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images. A copy of the written consent has been submitted to this journal.
Figures

Similar articles
-
Impact of halo-pelvic traction duration on pulmonary improvement quantified by pulmonary function tests and three-dimensional lung reconstruction in severe rigid kyphoscoliosis: a prospective cohort study.J Orthop Surg Res. 2025 Jul 26;20(1):705. doi: 10.1186/s13018-025-06126-y. J Orthop Surg Res. 2025. PMID: 40713841 Free PMC article.
-
Tri-cortical pedicle screw fixation in the most cranial instrumented segment to prevent proximal junctional kyphosis.Spine J. 2025 Aug;25(8):1698-1707. doi: 10.1016/j.spinee.2025.02.002. Epub 2025 Feb 22. Spine J. 2025. PMID: 39993503
-
Patient and surgical predictors of 3D correction in posterior spinal fusion: a systematic review.Eur Spine J. 2023 Jun;32(6):1927-1946. doi: 10.1007/s00586-023-07708-2. Epub 2023 Apr 20. Eur Spine J. 2023. PMID: 37079078
-
Posterior vertebral column resection in spinal deformity: a systematic review.Eur Spine J. 2016 Aug;25(8):2368-75. doi: 10.1007/s00586-015-3767-7. Epub 2015 Jan 20. Eur Spine J. 2016. PMID: 25599850
-
Posterior vertebral column resection with preservation of posterior ligamentous complex for severe angular spinal kyphotic deformity: a comparative study.Eur Spine J. 2025 Jul;34(7):2847-2855. doi: 10.1007/s00586-025-08910-0. Epub 2025 May 17. Eur Spine J. 2025. PMID: 40381021
References
-
- Sheehan, D. D. & Grayhack, J. Pediatric scoliosis and kyphosis: an overview of diagnosis, management, and surgical treatment. Pediatr. Ann.46 (12), e472–e480 (2017). - PubMed
-
- Kempen, D. et al. Pulmonary function in children and adolescents with untreated idiopathic scoliosis: a systematic review with meta-regression analysis. Spine J.22 (7), 1178–1190 (2022). - PubMed
-
- Bouchoucha, S. et al. Progressive correction of severe spinal deformities with halo-gravity traction. Acta Orthop. Belg.77 (4), 529–534 (2011). - PubMed
-
- Sucato, D. J. Management of severe spinal deformity: scoliosis and kyphosis. Spine (Phila Pa. 1976). 35 (25), 2186–2192 (2010). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
