

Impact of SGLT2 inhibitors on myocardial fibrosis in diabetic HFpEF: a longitudinal study
- PMID: 40624547
- PMCID: PMC12235812
- DOI: 10.1186/s40001-025-02834-7
Impact of SGLT2 inhibitors on myocardial fibrosis in diabetic HFpEF: a longitudinal study
Abstract
Background: Sodium-glucose co-transporter 2 (SGLT2) inhibitors offer cardiovascular benefits in patients with heart failure, yet their direct effects on myocardial fibrosis-particularly in heart failure with preserved ejection fraction (HFpEF) and type 2 diabetes (T2D)-remain underexplored. This study investigates the antifibrotic impact of dapagliflozin in diabetic HFpEF patients, with a focus on its potential as a disease-modifying therapy.
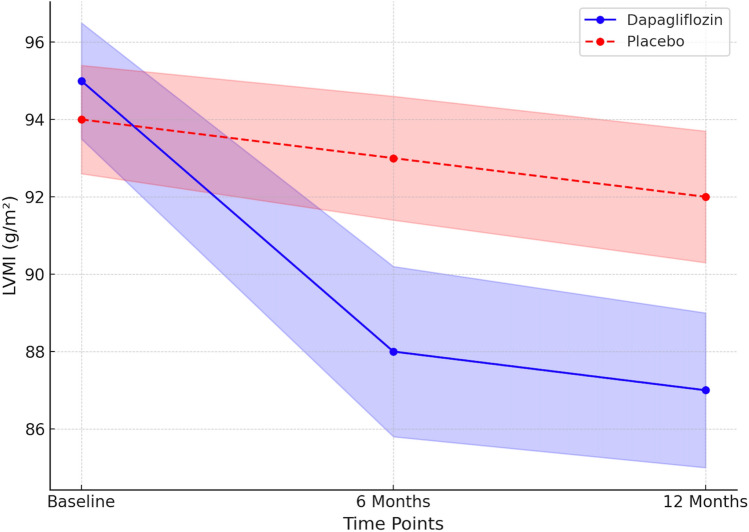
Methods: In a multicenter, double-blind, placebo-controlled trial, 100 patients with HFpEF and T2D were randomized (1:1) to receive dapagliflozin 10 mg daily or placebo for 12 months. Stratification was performed by baseline extracellular volume fraction (ECV). Myocardial fibrosis was assessed using cardiac MRI-derived ECV at baseline, 6 months, and 12 months. Secondary endpoints included changes in left ventricular mass index (LVMI), HbA1c, and 6-min walk test (6MWT) distance.
Results: Dapagliflozin significantly reduced myocardial fibrosis (mean ΔECV: - 3.5% [95% CI - 4.2 to - 2.8]) compared to placebo (- 0.8% [95% CI - 1.3 to - 0.4]; p < 0.001). Additional benefits included greater reductions in LVMI (- 8.2 g/m2 vs. - 2.1 g/m2; p = 0.002), improved glycemic control (HbA1c: - 1.2% vs. - 0.4%; p = 0.01), and enhanced functional capacity (+ 45 m vs. + 10 m in 6MWT; p = 0.01).
Conclusions: Dapagliflozin demonstrated a significant reduction in myocardial fibrosis and improvements in cardiac structure, metabolic control, and exercise tolerance in HFpEF patients with T2D. These findings support the evolving role of SGLT2 inhibitors as validated components of guideline-directed therapy, with potential disease-modifying effects through targeted myocardial fibrosis regression.
Keywords: Cardiac MRI; Dapagliflozin; HFpEF; Myocardial fibrosis; SGLT2 inhibitors; Type 2 diabetes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board (IRB # 0075–22-FB). Competing interests: The authors declare no competing interests.
Figures




References
-
- Gevaert AB, Van De Bruaene A, Van Mieghem NM, et al. Heart failure with preserved ejection fraction: recent concepts in diagnosis, mechanisms, and management. Heart. 2022;108(17):1342–50. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
