

Cost-effectiveness of dabigatran for thromboembolic events prevention in atrial fibrillation patients in Chile
- PMID: 40624582
- PMCID: PMC12235837
- DOI: 10.1186/s12962-025-00642-8
Cost-effectiveness of dabigatran for thromboembolic events prevention in atrial fibrillation patients in Chile
Abstract
Background: Atrial fibrillation (AF) is the most common sustained arrhythmia in adults, associated with significant morbidity, mortality, and economic burden due to thromboembolic events. In Chile, acenocoumarol is the most widely used anticoagulant, while access to direct oral anticoagulants (DOACs) such as dabigatran, rivaroxaban, and apixaban remains limited for AF patients. Among DOACs, dabigatran is the only one with an approved specific reversal agent (idarucizumab) available in the Chilean public system. Evaluating the cost-effectiveness of these alternatives is critical for informing resource allocation.
Aims: To evaluate the cost-effectiveness of dabigatran compared to acenocoumarol, rivaroxaban and apixaban, for thromboembolic events prevention in atrial fibrillation (AF) patients, from the Chilean public health payer perspective.
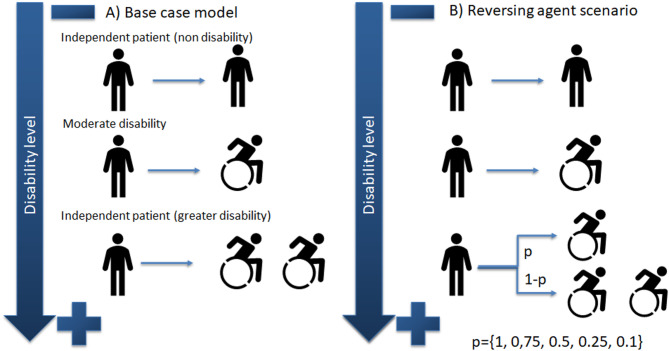
Methods: A Markov cohort model was used to represent the natural history of AF in terms of ischemic and hemorrhagic complications. Direct costs were obtained from local official sources and converted to US dollars (1 USD = 710.9 CLP at 2022). Data about major events and utilities were obtained from the literature. We applied an undifferentiated discount rate of 3% for costs and outcomes over a lifetime time horizon. Uncertainty was characterized through deterministic and probabilistic sensitivity analysis. We also examined the use of idarucizumab and prothrombin-complexes-concentrate (PCC) as reversal agents in an emergency setting as an additional scenario-analysis.
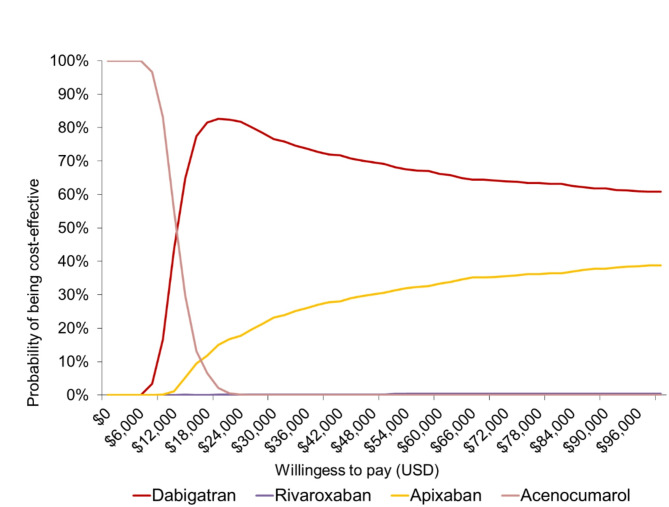
Results: Dabigatran was the most (cost-)effective among all alternatives (8.53 QALYs). Considering the Chilean cost-effectiveness threshold of USD 17,200 (1 GDP per capita), dabigatran was cost-effective (USD 11,042 per QALY gained), while both rivaroxaban and apixaban were dominated by dabigatran. Regarding the second-order uncertainty, at the suggested threshold, dabigatran exhibit the highest probability of being cost-effective (approximately 60%). In the reversal agent scenario, dabigatran plus idarucizumab was also found to be cost-effective in the Chilean context.
Conclusion: Dabigatran is cost-effective and dominates both rivaroxaban and apixaban at current publicly available prices in Chile. In addition, we expect dabigatran-idarucizumab is also expected to be cost-effective for Chilean health system when is compared against acenocoumarol-PCC as reversal agents.
Keywords: Atrial fibrillation; Cost-effectiveness; Dabigatran; Thromboembolic events.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. JAMA. 2001;285(18):2370–5. - PubMed
-
- Gallagher C, Hendriks JM, Middeldorp ME, Elliott AD, Lau DH, Sanders P. Reducing the burden of atrial fibrillation cost: is integrated care the answer?? Can J Cardiol. 2019;35(9):1094–6. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
