

Patterns of emergency dispatch calls and their changes during the COVID-19 pandemic in Ulaanbaatar, Mongolia
- PMID: 40624622
- PMCID: PMC12235795
- DOI: 10.1186/s12873-025-01273-1
Patterns of emergency dispatch calls and their changes during the COVID-19 pandemic in Ulaanbaatar, Mongolia
Abstract
Background: Emergency medical dispatch is a crucial component of a national healthcare system. This study provides the first comprehensive analysis of the temporal patterns of emergency medical service evaluations in Ulaanbaatar, Mongolia, and evaluates the impact of COVID-19 lockdowns on those patterns.
Methods: We analyzed emergency medical evaluations recorded by physicians following the dispatch calls received by the Emergency Medical Communication Center in Ulaanbaatar between 2016 and 2021. We assessed trends in the number of emergency calls, demographic distributions, and temporal patterns. Comparative analysis was conducted to assess the impact of COVID-19 lockdowns, with a focus on seasonal, weekly, and hourly variations.
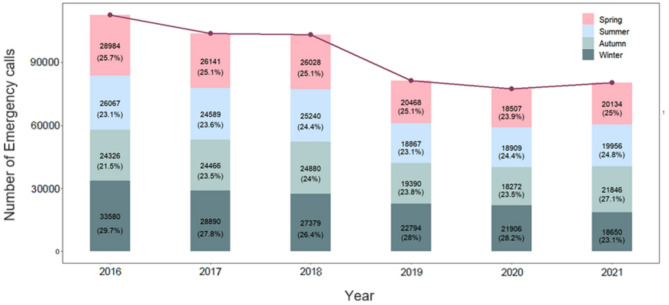
Results: There were 558,457 emergency calls during the study period, and a total of 8 diagnoses (I, J, Y, F, K, G, O, and Z according to ICD-10) constituted 99.1% of the emergency calls. The two most abundant causes for emergency calls in Ulaanbaatar are “Diseases of the circulatory system (I)” and “Diseases of the respiratory system (J)” in all seasons. We analyzed the temporal patterns of the calls and identified that the highest number of calls was received in winter, weekends, and evenings for the total number of calls. Further, we conducted an analysis of calls during COVID-19 strict lockdown periods. A retrospective analysis of the impacts of the COVID-19 pandemic on emergency calls showed that emergency calls decreased by 24% compared to the previous year. Notably, the difference between the COVID-19 strict lockdown period and the preceding period was more pronounced during periods of strict lockdown implementation.
Conclusions: This is the first comprehensive analysis of EMS calls in Ulaanbaatar from 2016 to 2021, providing valuable insights into both long-term temporal trends and the effects of pandemic-related lockdowns. These findings can support improved EMS planning and inform public health policies in low- and middle-income countries.
Clinical trial number: Not applicable.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12873-025-01273-1.
Keywords: COVID-19 impact; Emergency calls; Emergency medical communication center; Mongolia; Temporal analysis; Ulaanbaatar.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethical committee of the “Ach” Medical Univeristy (decision 2023/A3 from 6 May 2023), however the consent was deemed unnecessary according to national legislation (Law of Mongolia on Personal Data Protection, 2021). The data was anonymized and treated with the utmost confidentiality in accordance with applicable Mongolia laws. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Changes in handwashing knowledge, attitudes, and practices among primary schoolchildren in Ulaanbaatar, Mongolia during the COVID-19 pandemic.Front Public Health. 2025 Jun 12;13:1570178. doi: 10.3389/fpubh.2025.1570178. eCollection 2025. Front Public Health. 2025. PMID: 40575101 Free PMC article.
-
A pilot study on feasibility and hypothesis exploration: reducing on-scene length of stay of the emergency teams via ambulance dispatch teleconsultation for prehospital examination.Einstein (Sao Paulo). 2025 May 12;23:eAO1469. doi: 10.31744/einstein_journal/2025AO1469. eCollection 2025. Einstein (Sao Paulo). 2025. PMID: 40367011 Free PMC article. Clinical Trial.
-
Video livestreaming in emergency trauma dispatch: an observational study of technological integration with clinical decision-making in prehospital enhanced care services.Scand J Trauma Resusc Emerg Med. 2025 Jun 19;33(1):108. doi: 10.1186/s13049-025-01406-2. Scand J Trauma Resusc Emerg Med. 2025. PMID: 40537850 Free PMC article.
-
Recognition of out-of-hospital cardiac arrest during emergency calls - a systematic review of observational studies.Scand J Trauma Resusc Emerg Med. 2017 Feb 1;25(1):9. doi: 10.1186/s13049-017-0350-8. Scand J Trauma Resusc Emerg Med. 2017. PMID: 28143588 Free PMC article.
-
The prevalences, changes, and related factors of child maltreatment during the COVID-19 pandemic: A systematic review.Child Abuse Negl. 2023 Jan;135:105992. doi: 10.1016/j.chiabu.2022.105992. Epub 2022 Dec 16. Child Abuse Negl. 2023. PMID: 36549089 Free PMC article.
References
-
- Kobusingye OC, Hyder AA, Bishai D, Joshipura M, Hicks ER, Mock C. Emergency Medical Services. International bank for reconstruction and Development/The World Bank; 2006. - PubMed
-
- Martin RJ, Mousavi R, Saydam C. Predicting emergency medical service call demand: a modern spatiotemporal machine learning approach. Oper Res Health Care [Internet]. 2021;28(100285):100285. Available from: 10.1016/j.orhc.2021.100285
-
- Vargas Román MI, de Miguel ÁG, Garrido PC, et al. Epidemiologic intervention framework of a prehospital emergency medical service. Prehosp Emerg Care. 2005;9(3):344–54. 10.1080/10903120590962157. - PubMed
LinkOut - more resources
Full Text Sources
