

Evaluated anatomical variations in children by sacrococcygeal ultrasonography as a new tool: a report from a Chinese tertiary hospital
- PMID: 40624908
- PMCID: PMC12239231
- DOI: 10.1080/07853890.2025.2528977
Evaluated anatomical variations in children by sacrococcygeal ultrasonography as a new tool: a report from a Chinese tertiary hospital
Abstract
Objective: Anatomical variations in the sacrococcygeal region can lead to complications such as accidental dural puncture during caudal block. This study aimed to determine the prevalence of sacrococcygeal anatomical variations using ultrasonography and to evaluate the necessity of ultrasound guidance in sacral block procedures.
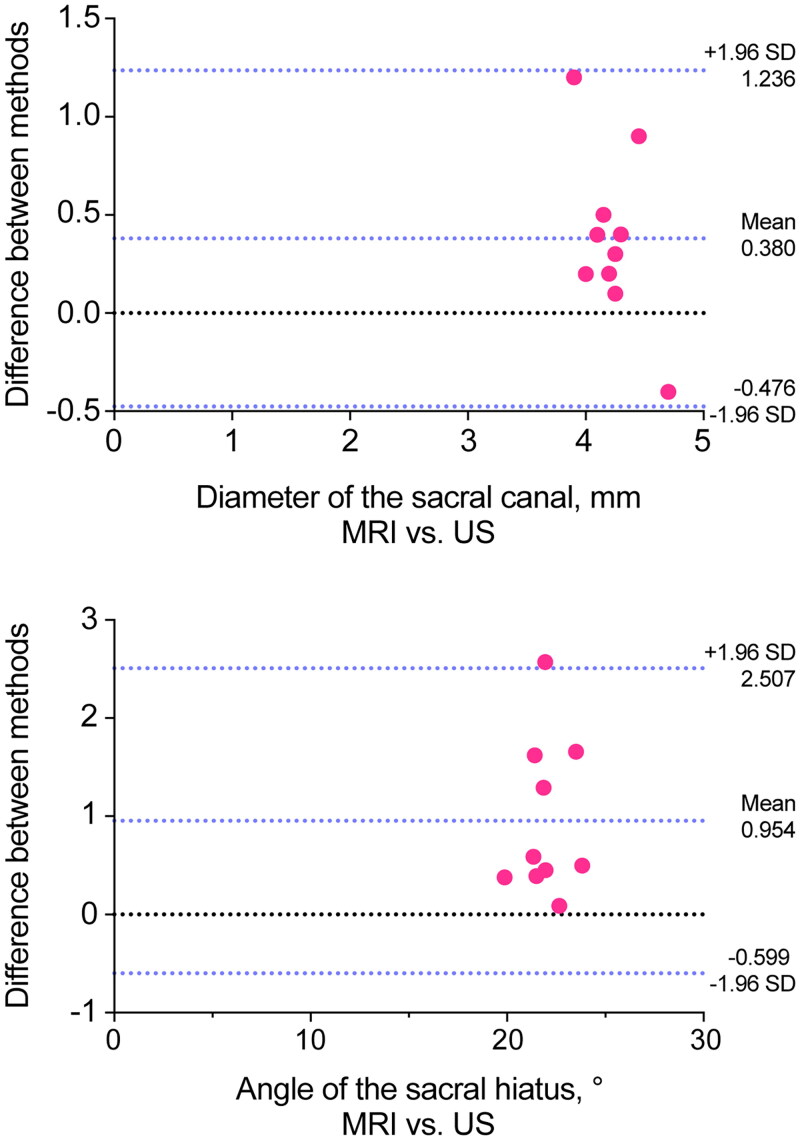
Methods: Ultrasound findings of sacrococcygeal anatomy were validated against magnetic resonance imaging (MRI). A detailed ultrasound protocol was subsequently applied to assess sacrococcygeal anatomy in pediatric patients.
Results: Ultrasound and MRI demonstrated strong concordance in evaluating sacrococcygeal anatomy. The most common anatomical variation was a low-lying dural sac (16.2%), followed by incomplete sacral cornua (4.9%). The dural sac termination level was inversely associated with age (odds ratio: 0.996, 95% CI: 0.945-0.987; p < 0.001). Other variations included abnormal coccyx curvature (4.3%), sacral skewness (3.8%), and sacral hiatus atresia (1.1%), with no pathological abnormalities detected.
Conclusion: Comprehensive ultrasound scanning effectively identifies anatomical variations in the sacrococcygeal region of pediatric patients, which are highly prevalent. Routine preprocedural ultrasound examinations and ultrasound guidance during caudal block procedures are strongly recommended to enhance safety and accuracy.
Keywords: Caudal block; magnetic resonance imaging; sacrococcygeal anatomical variations; ultrasound.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures



Similar articles
-
Ultrasonography-guided catheter-over-needle insertion for caudal epidural catheter placement in adults: technical considerations.BMC Anesthesiol. 2025 Apr 1;25(1):149. doi: 10.1186/s12871-025-02889-3. BMC Anesthesiol. 2025. PMID: 40169958 Free PMC article.
-
Ultrasound guidance versus anatomical landmarks for neuraxial anaesthesia in adults.Cochrane Database Syst Rev. 2025 May 27;5(5):CD014964. doi: 10.1002/14651858.CD014964.pub2. Cochrane Database Syst Rev. 2025. PMID: 40421607
-
The use of ultrasound guidance for perioperative neuraxial and peripheral nerve blocks in children.Cochrane Database Syst Rev. 2016 Feb 19;2(2):CD011436. doi: 10.1002/14651858.CD011436.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2019 Feb 27;2:CD011436. doi: 10.1002/14651858.CD011436.pub3. PMID: 26895372 Free PMC article. Updated.
-
MRI software and cognitive fusion biopsies in people with suspected prostate cancer: a systematic review, network meta-analysis and cost-effectiveness analysis.Health Technol Assess. 2024 Oct;28(61):1-310. doi: 10.3310/PLFG4210. Health Technol Assess. 2024. PMID: 39367754 Free PMC article.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources