

Exclusion-based exome sequencing in critically ill adults 18-40 years old has a 24% diagnostic rate and finds racial disparities in access to genetic testing
- PMID: 40628270
- PMCID: PMC12414659
- DOI: 10.1016/j.ajhg.2025.06.007
Exclusion-based exome sequencing in critically ill adults 18-40 years old has a 24% diagnostic rate and finds racial disparities in access to genetic testing
Abstract
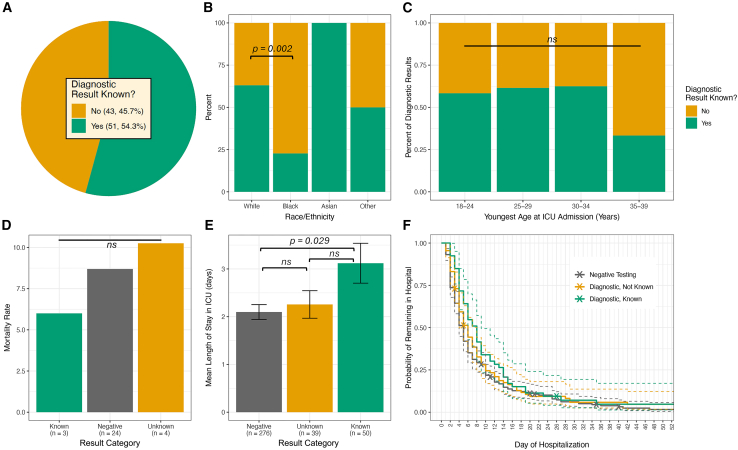
Despite the well-documented benefits of genome sequencing in critically ill pediatric patients, genomic testing is rarely utilized in critically ill adults, and data on its diagnostic yield and clinical implications in this population are lacking. We retrospectively analyzed whole-exome sequencing (WES) data from 365 adults ages 18-40 years with intensive care unit (ICU) admissions at the University of Pennsylvania Health System. For each participant, two medical genetics- and internal medicine-trained clinicians reviewed WES reports and patient charts for variant classification, result interpretation, and identification of genetic diagnoses related to their critical illness. We identified a diagnostic genetic variant in 24.4% of patients, with nearly half of these being unknown to patients and their care teams at the time of ICU admission. Of these genetic diagnoses, 76.6% conferred specific care-altering medical management recommendations. Importantly, diagnostic yield did not decrease with increasing patient age, and patients with undocumented diagnoses trended toward higher mortality rates compared to either patients with known diagnoses or patients with negative exomes. Significant disparities were seen by electronic health record-reported race, with genetic diagnoses known/documented for 63.1% of White patients at the time of ICU admission but only for 22.7% of Black patients. Altogether, the results of this study of broad, exclusion-based genetic testing in the critically ill adult population suggest that the broad implementation of genetic testing in critically ill adults has the potential to improve patient care and dismantle disparities in healthcare delivery.
Keywords: adult genetics; critical illness; disparities; exome; genetics.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures





References
-
- Krantz I.D., Medne L., Weatherly J.M., Wild K.T., Biswas S., Devkota B., Hartman T., Brunelli L., Fishler K.P., et al. NICUSeq Study Group Effect of Whole-Genome Sequencing on the Clinical Management of Acutely Ill Infants With Suspected Genetic Disease: A Randomized Clinical Trial. JAMA Pediatr. 2021;175:1218–1226. doi: 10.1001/jamapediatrics.2021.3496. - DOI - PMC - PubMed
-
- Dimmock D., Caylor S., Waldman B., Benson W., Ashburner C., Carmichael J.L., Carroll J., Cham E., Chowdhury S., Cleary J., et al. Project Baby Bear: Rapid precision care incorporating rWGS in 5 California children’s hospitals demonstrates improved clinical outcomes and reduced costs of care. Am. J. Hum. Genet. 2021;108:1231–1238. doi: 10.1016/j.ajhg.2021.05.008. - DOI - PMC - PubMed
-
- Olde Keizer R.A.C.M., Marouane A., Kerstjens-Frederikse W.S., Deden A.C., Lichtenbelt K.D., Jonckers T., Vervoorn M., Vreeburg M., Henneman L., de Vries L.S., et al. Rapid exome sequencing as a first-tier test in neonates with suspected genetic disorder: results of a prospective multicenter clinical utility study in the Netherlands. Eur. J. Pediatr. 2023;182:2683–2692. doi: 10.1007/s00431-023-04909-1. - DOI - PMC - PubMed
-
- Lunke S., Eggers S., Wilson M., Patel C., Barnett C.P., Pinner J., Sandaradura S.A., Buckley M.F., Krzesinski E.I., et al. Australian Genomics Health Alliance Acute Care Flagship Feasibility of Ultra-Rapid Exome Sequencing in Critically Ill Infants and Children With Suspected Monogenic Conditions in the Australian Public Health Care System. JAMA. 2020;323:2503–2511. doi: 10.1001/jama.2020.7671. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
