

Fascial incision shapes and paracolostomy hernia: cruciate vs. reinforced longitudinal (the "Hepworth hitch"): longcross randomized controlled trial (GECO2 STUDY)
- PMID: 40629015
- PMCID: PMC12238066
- DOI: 10.1007/s00384-025-04939-1
Fascial incision shapes and paracolostomy hernia: cruciate vs. reinforced longitudinal (the "Hepworth hitch"): longcross randomized controlled trial (GECO2 STUDY)
Abstract
Purpose: Primary objective was to compare the rates of parastomal hernia (PH) at 2 years after the creation of a terminal colostomy using two types of fascial incision: cross-shaped and reinforced longitudinal. Secondary objectives included the evaluation of postoperative complications, readmissions, reoperations for PH, and patients' quality of life.
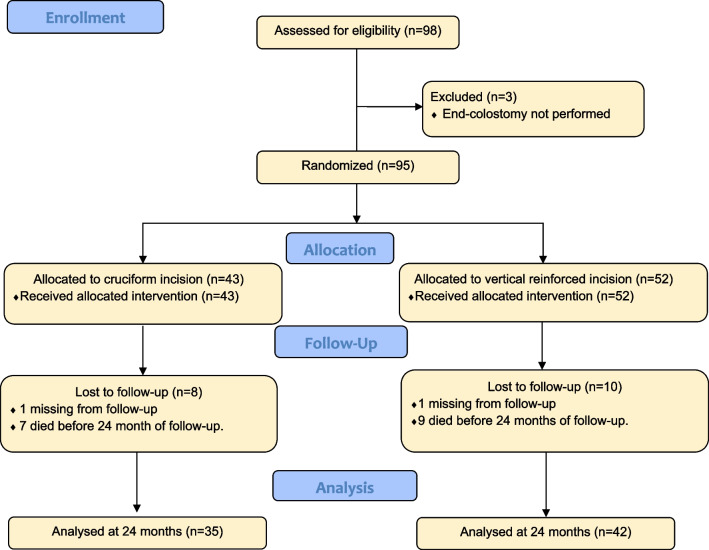
Methods: This was a multicenter superiority clinical trial conducted at 5 hospitals involving patients with rectal cancer and definitive colostomy. Patients were randomized into two groups: cross incision (n = 42) or reinforced longitudinal incision (n = 52), for the exteriorization of the colon in terminal colostomy. PH at 2 years was determined by physical examination, computed tomography (CT), and symptoms. Baseline data on risk factors for PH, postoperative complications, readmissions, reoperations for symptomatic PH, and quality of life were recorded.
Results: A total of 95 patients were included: cross (n = 42) and reinforced longitudinal (n = 52). Demographic characteristics, risk factors for PH, and surgical factors were similar between the two groups. No significant differences were found in the clinical PH rate between the cruciate versus longitudinal incision groups (48.60% vs. 45.20%; p = 0.770), radiological PH (54.30% vs. 53.70%; p = 0.956), or symptomatic PH (14.30% vs. 19%; p = 0.579). The comprehensive complication index (CCI), readmissions, and reoperation rates for symptomatic PH (8.6% vs. 7.1%; p = 0.816) were similar in both groups. No significant differences were observed in the three health aspects evaluated using the EORTC QLQ-C30 scale.
Conclusion: The reinforcement of a longitudinal fascial incision as an isolated surgical technique does not reduce the incidence of PH after a 2-year follow-up.
Keywords: Fascial incision shapes; Paracolostomy hernia; Terminal colostomy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests : GP is Editor on the Journal but was not involved in any way in the Editorial peer review process of this article.
References
-
- ACPGBI Parastomal Hernia Group (2018) Prevention and treatment of parastomal hernia: a position statement on behalf of the Association of Coloproctology of Great Britain and Ireland. Colorectal Dis 20(S2):5–19 - PubMed
-
- Carne PWG, Robertson GM, Frizelle FA (2003) Parastomal hernia. Br J Surg 90(7):784–793 - PubMed
-
- Cingi A, Cakir T, Sever A, Aktan AO (2006) Enterostomy site hernias: a clinical and computerized tomographic evaluation. Dis Colon Rectum 49(10):1559–1563 - PubMed
-
- Andersen RM, Klausen TW, Danielsen AK, Vinther A, Gögenur I, Thomsen T (2018) Incidence and risk factors for parastomal bulging in patients with ileostomy or colostomy: a register-based study using data from the Danish Stoma Database Capital Region. Colorectal Dis 20(4):331–340 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
