

Intra-hospital transport of adult critically ill patients treated with high flow nasal cannula oxygen: a prospective observational multicenter study
- PMID: 40629187
- PMCID: PMC12238688
- DOI: 10.1186/s13613-025-01502-7
Intra-hospital transport of adult critically ill patients treated with high flow nasal cannula oxygen: a prospective observational multicenter study
Abstract
Background: Acute respiratory failure is a common reason for admission to the intensive care unit, and patients are frequently treated with high-flow nasal cannula oxygen therapy (HFNC). Intra-hospital transport of critically ill patients, such as between hospital wards and the intensive care unit or for diagnostic exams, is common. Transportable HFNC can be used during these intra-hospital transports. We aimed to evaluate the complications associated with intra-hospital transport of patients treated with HFNC.
Methods: We conducted a prospective, descriptive multicenter study between May 2022 and May 2024, involving critically ill adult patients who were treated with HFNC prior to transport and required intra-hospital transport for any reason, accompanied by an intensive care unit team. The primary objective was to evaluate the incidence of severe adverse events including severe hypoxemia (with pulse oxygen saturation of less than 80%), need for intubation, need for non-invasive ventilation or cardiorespiratory arrest during transport. Secondary objectives were to assess the incidence of non-severe adverse events, defined as the need for increased inspired oxygen fraction, switching HFNC for standard oxygen therapy, nasal cannula removal or dysfunction of the HFNC device.
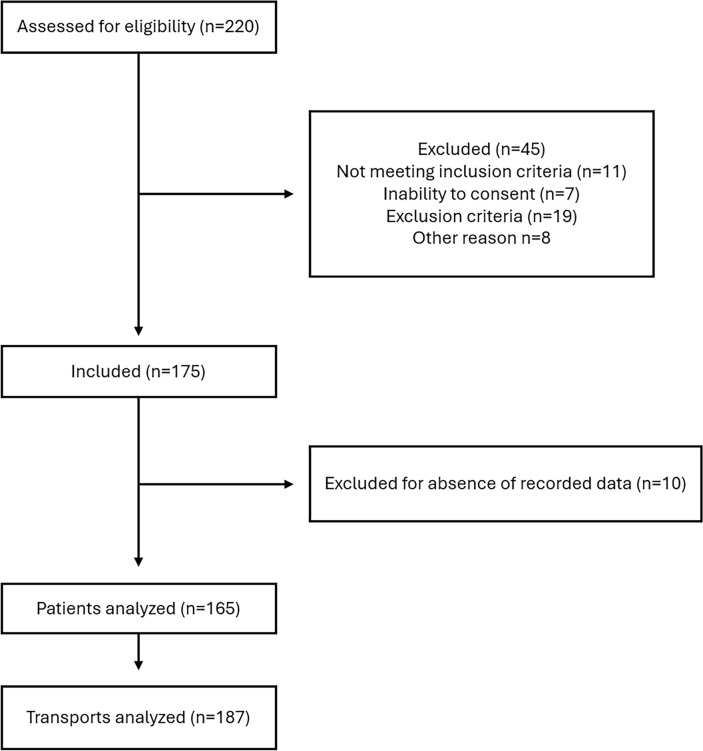
Results: We included 165 patients and analyzed 187 transports. Eight (4.3%) severe adverse events occurred in 7 patients including 6 cases of severe transient hypoxemia and 2 cases of non-invasive ventilation. All of them were transient severe hypoxemia that occurred during the first transport. Forty-three (23%) non-severe adverse events occurred, including 29(15.6%) cases of increased inspired oxygen fraction requirement, 7/187 (3.74%) cases of nasal cannula removal, 6/187 (3.2%) cases of HFNC device dysfunction, and 1 (0.5%) case involved replacing HFNC with standard oxygen therapy.
Conclusion: HFNC during intra-hospital transport of critically ill patients had a low incidence of severe adverse events. Non-severe adverse events were more frequent, but their potential impact could not be assessed in this study and warrants further investigation.
Trial registration: Clinicalstrials.gov, NCT05311007, registered 23 March 2022, https://clinicaltrials.gov/study/NCT05311007?term=hospiflow&rank=1 .
Keywords: Critical ill patient; High flow nasal cannula; Intensive care unit; Intra-hospital transport; Oxygenation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the French Ethics Committee (Comité de Protection des Personnes—Ile de France VI—No. 22.00476.000051) on March 8, 2022, and enregistered at Clinicaltrials.gov (NCT05311007) and was conducted in compliance with the latest version of the Declaration of Helsinki and good clinical practice guidelines. Patients, or, if they were unable to provide consent, their next of kin gave oral informed consent. Consent for publication: Not applicable. Competing interests: MAN reports receiving remuneration for presentations, fundings and material support from Fisher & Paykel healthcare and travel and congress fees from Pfizer. However, Fisher & Paykel healthcare was not involved in the development, writing, or submission of the present manuscript. The other authors declared no conflicts of interest.
Figures
References
-
- Behrendt CE. Acute respiratory failure in the United States: incidence and 31-day survival. Chest. 2000;118:1100–5. - PubMed
-
- Mauri T, Turrini C, Eronia N, Grasselli G, Volta CA, Bellani G, et al. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. 2017;195:1207–15. - PubMed
-
- Lahner D, Nikolic A, Marhofer P, Koinig H, Germann P, Weinstabl C, et al. Incidence of complications in intrahospital transport of critically ill patients–experience in an Austrian university hospital. Wien Klin Wochenschr. 2007;119:412–6. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
