

A scoring model integrating CXCL9, GDF15, FGF21, and NfL, predicts long-term mortality in type 2 diabetes: a retrospective study
- PMID: 40629349
- PMCID: PMC12239483
- DOI: 10.1186/s12933-025-02830-5
A scoring model integrating CXCL9, GDF15, FGF21, and NfL, predicts long-term mortality in type 2 diabetes: a retrospective study
Abstract
Background: Type 2 diabetes (T2D) is a chronic metabolic disorder associated with aging, systemic inflammation, and increased long-term mortality. Identifying prognostic biomarkers may improve risk stratification and guide personalized interventions. This study aimed to evaluate the long-term prognostic value of circulating biomarkers related to inflammation, metabolic stress, and organ damage in individuals with T2D.
Methods: A retrospective study was conducted on a cohort of 478 individuals with T2D, followed for a median of 16.1 years. Ten circulating biomarkers (IL-6, IL-10, CD163, CXCL9, CCL22, GDF15, IL-33, FGF21, Follistatin, and neurofilament light chain [NfL]) were quantified using an automated immunoassay platform. Kaplan-Meier survival analysis and Cox proportional hazards models were used to assess their prognostic significance for all-cause mortality. A biomarker-based scoring model was developed by integrating independent predictors of mortality. Predictive performance was evaluated in comparison with the RECODe equation, a validated risk model for diabetes complications and mortality.
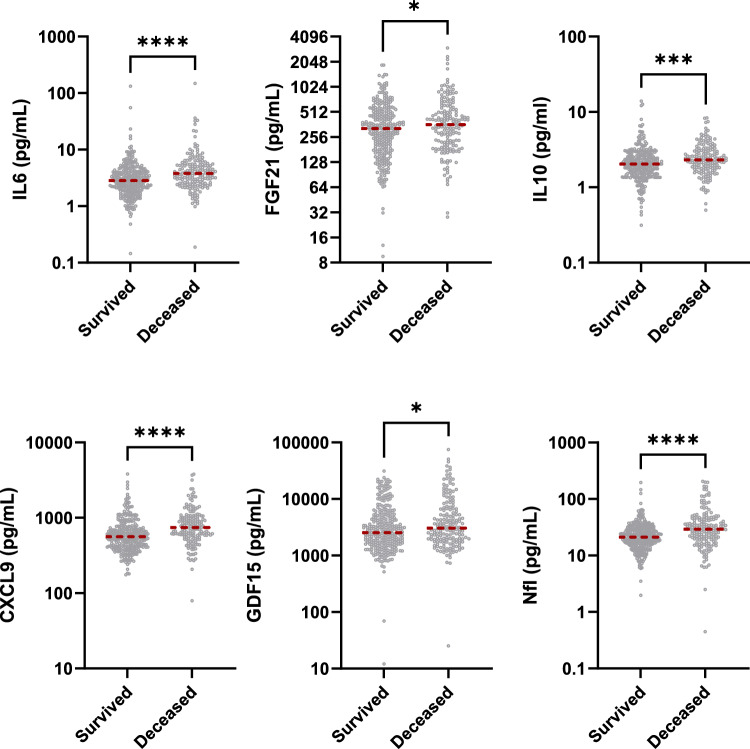
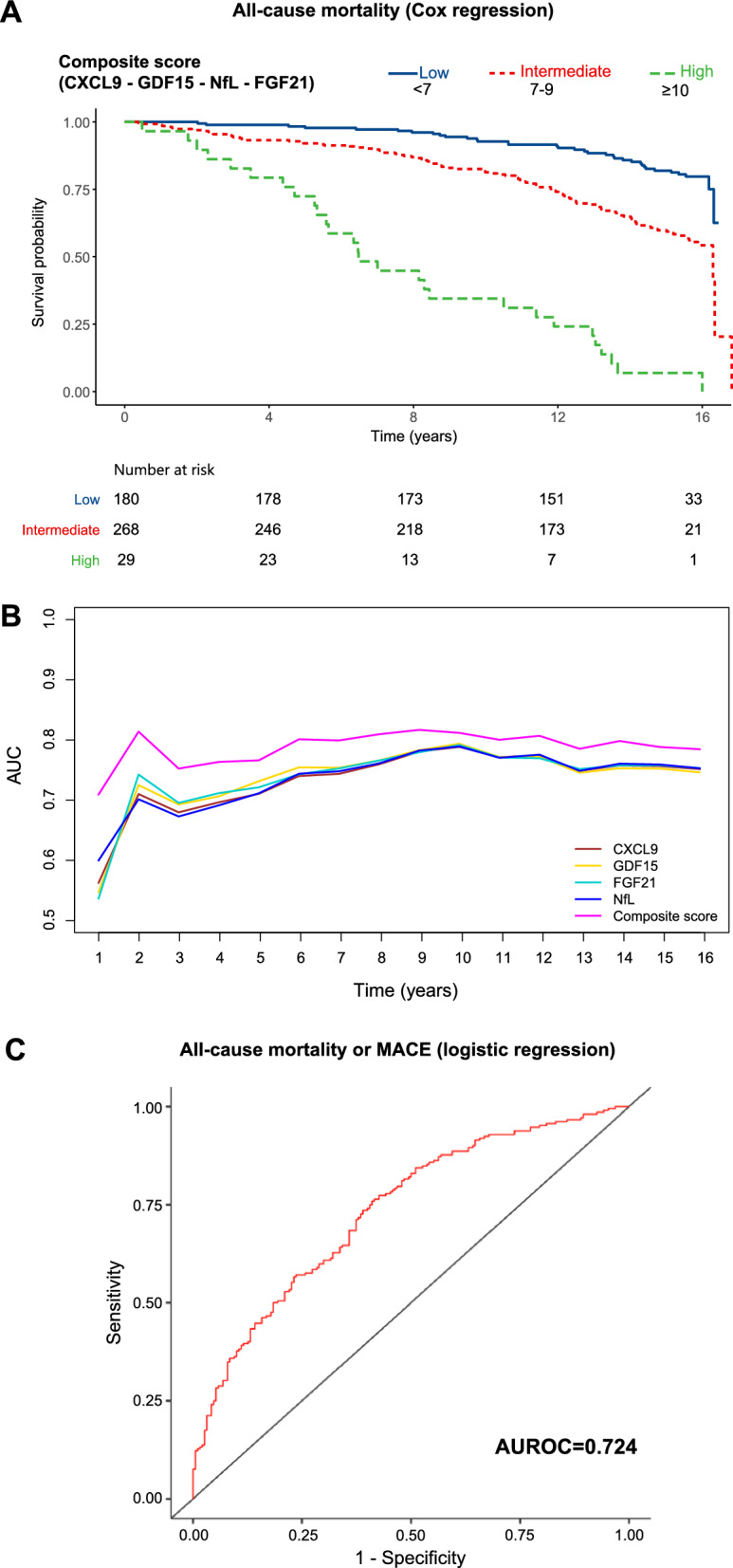
Results: Deceased individuals exhibited significantly higher levels of IL-6, IL-10, CXCL9, FGF21, NfL, and GDF15. Biomarker levels correlated with both microvascular and macrovascular complications, particularly neuropathy, nephropathy, retinopathy, and major adverse cardiovascular events (MACE). In multivariable Cox regression analysis, four biomarkers emerged as independent predictors of mortality: CXCL9 (HR per 1 SD increase 1.19, 95% CI 1.05-1.36, p = 0.006), GDF15 (HR 1.16, 95% CI 1.02-1.33, p = 0.032), NfL (HR 1.25, 95% CI 1.09-1.43, p = 0.001), and FGF21 (HR 1.20, 95% CI 1.04-1.37, p = 0.009). A composite biomarker score (range: 4-12) stratified individuals into distinct risk categories, with each 1-point increase in the score associated with a 55% higher mortality risk (HR 1.53, 95% CI 1.35-1.74, p < 0.001). The biomarker score remained independently predictive after adjusting for clinical covariates and significantly improved individual-level risk classification beyond the RECODe model, as demonstrated by net reclassification and discrimination improvement metrics.
Conclusions: These findings suggest that inflammatory and metabolic stress-related biomarkers independently predict long-term mortality in T2D. The biomarker-based scoring model enhances risk stratification and improves the prognostic performance of existing clinical tools, such as the RECODe equation, potentially informing targeted clinical interventions.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study received approval from the Institutional Review Board of IRCCS INRCA hospital (Approval No. 34/CdB/03). Written informed consent was obtained from all participants in compliance with the principles outlined in the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Marx N, Federici M, Schutt K, Muller-Wieland D, Ajjan RA, Antunes MJ, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043–140. - PubMed
-
- Prattichizzo F, Giuliani A, Sabbatinelli J, Matacchione G, Ramini D, Bonfigli AR, et al. Prevalence of residual inflammatory risk and associated clinical variables in patients with type 2 diabetes. Diabetes Obes Metab. 2020;22(9):1696–700. - PubMed
MeSH terms
Substances
Grants and funding
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
- Ricerca corrente/Ministero della Salute
LinkOut - more resources
Full Text Sources
Medical
Research Materials
