

Three-port laparoscopic cholecystectomy in situs inversus totalis: A case report
- PMID: 40629628
- PMCID: PMC12237338
- DOI: 10.1097/MD.0000000000043186
Three-port laparoscopic cholecystectomy in situs inversus totalis: A case report
Abstract
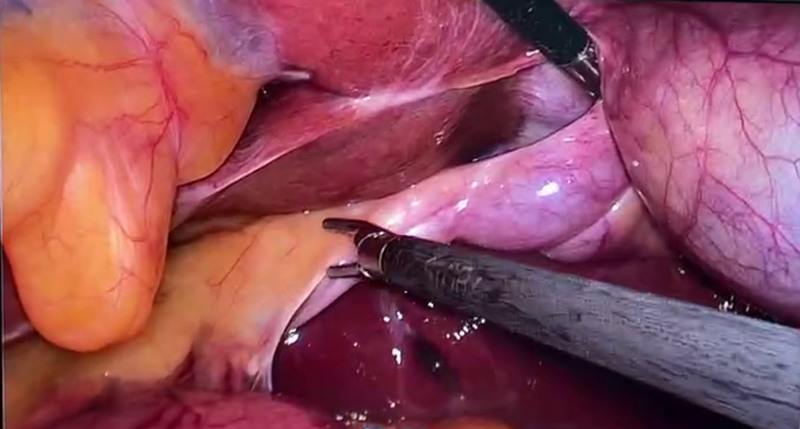
Rationale: Situs inversus totalis (SIT), a congenital anomaly characterized by the mirror-image inversion of thoracic and abdominal viscera, necessitates a cautious approach in the diagnosis and treatment of patients presenting with symptomatic cholelithiasis. Laparoscopic cholecystectomy, the preferred procedure for gallbladder removal in SIT patients, achieves favorable outcomes through thorough preoperative planning, a deep understanding of anatomy, and intraoperative adaptability.
Patient concerns: Herein, we present the case of a 51-year-old female patient in SIT who underwent a laparoscopic cholecystectomy without complications due to choledocholithiasis and gallbladder stones.
Diagnosis: Gallbladder stone; SIT.
Interventions: laparoscopic cholecystectomy.
Outcomes: No complications such as bleeding or bile leakage (after LC) was detected. The patient was discharged after 2 days and recovered well after 1-year follow-up.
Lessons: Thorough preoperative surgical planning, a deep understanding of anatomy, and the ability to adapt flexibly during surgery are key to the success of the operation.
Keywords: anatomical variations; laparoscopic cholecystectomy; situs inversus totalis.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures




References
-
- Chen W, Guo Z, Qian L, Wang L. Comorbidities in situs inversus totalis: a hospital‐based study. Birth Defects Res. 2020;112:418–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
