

Coexisting tubal pregnancy and intrauterine pregnancy during a natural pregnancy, first diagnosed via ultrasonography: A case report
- PMID: 40629650
- PMCID: PMC12237362
- DOI: 10.1097/MD.0000000000043148
Coexisting tubal pregnancy and intrauterine pregnancy during a natural pregnancy, first diagnosed via ultrasonography: A case report
Abstract
Rationale: The coexistence of intrauterine and extrauterine pregnancies is termed heterotopic pregnancy (HP). Most reported cases of HP occur after assisted reproductive technology, and HP in a natural pregnancy (NP) is very rare, often discovered intraoperatively. HP is a significant challenge for obstetricians, gynecologists, and sonographers.
Patient concerns: A 30-year-old nulliparous woman presented to the emergency department of a local tertiary hospital on day 66 of amenorrhea with abdominal pain, nausea, and vomiting without an obvious cause.
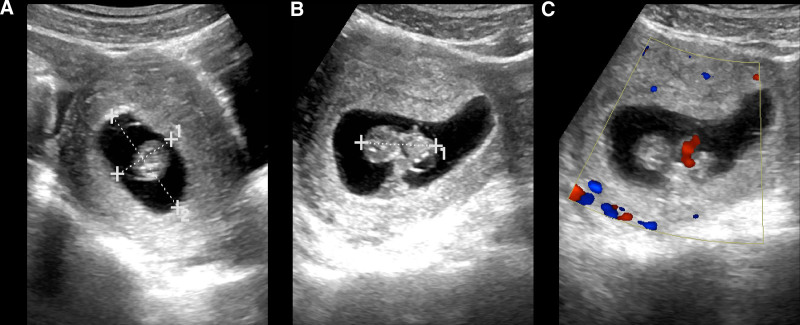
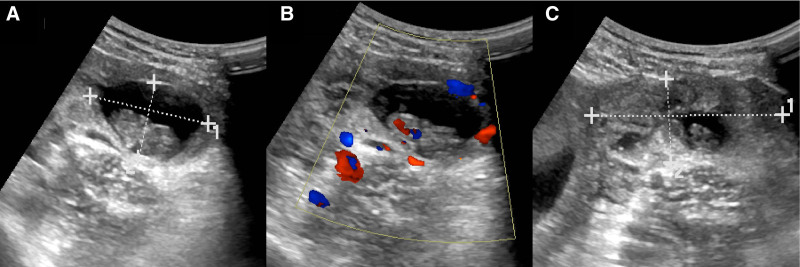
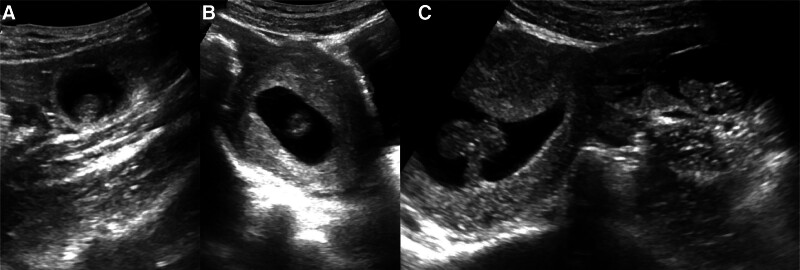
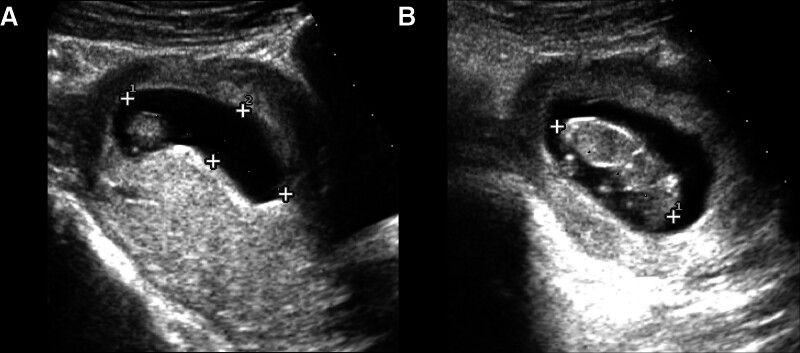
Diagnoses: Transabdominal gynecological ultrasonography revealed coexisting left ectopic pregnancy (EP) and intrauterine pregnancy (IP) in the NP, both with measurable fetal heart activity. In addition, abdominal fluid and extensive pelvic hematoma were observed.
Interventions: Given a ruptured EP with hemorrhage, the obstetrician-gynecologist performed an emergency surgery, finding approximately 500 mL of blood and blood clots in the abdominal and pelvic cavities. The left tubal ampullary segment was dilated and thickened, with a visible rupture and active bleeding. Therefore, the left fallopian tube was resected, and IP was managed with therapy.
Outcomes: The patient recovered well postoperatively and delivered a male infant by cesarean section at full term.
Lessons: The presence of IP does not exclude the coexistence of EP, even in NP. Although HP is rare and the symptoms of EP may not be obvious, sometimes masked by IP, obstetricians, gynecologists, and sonographers must remain vigilant in this regard to reduce the rate of missed diagnoses, provide early intervention, and safeguard the health of the pregnant woman and fetus.
Keywords: heterotopic pregnancy; intrauterine pregnancy; natural pregnancy; tubal pregnancy; ultrasonography.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Ruptured heterotopic pregnancy with successful term intrauterine pregnancy outcome after natural conception: a case report.J Med Case Rep. 2025 Jul 9;19(1):329. doi: 10.1186/s13256-025-05392-y. J Med Case Rep. 2025. PMID: 40635040 Free PMC article.
-
Intrauterine administration of human chorionic gonadotropin (hCG) for subfertile women undergoing assisted reproduction.Cochrane Database Syst Rev. 2016 May 20;(5):CD011537. doi: 10.1002/14651858.CD011537.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2018 Oct 20;10:CD011537. doi: 10.1002/14651858.CD011537.pub3. PMID: 27195724 Updated.
-
Endometrial injury for pregnancy following sexual intercourse or intrauterine insemination.Cochrane Database Syst Rev. 2022 Oct 24;10(10):CD011424. doi: 10.1002/14651858.CD011424.pub4. Cochrane Database Syst Rev. 2022. PMID: 36278845 Free PMC article.
-
Asynchronous development of bilateral tubal pregnancy after IVF-ET: A rare case report and review of the literature.Medicine (Baltimore). 2025 Aug 8;104(32):e43619. doi: 10.1097/MD.0000000000043619. Medicine (Baltimore). 2025. PMID: 40797486 Free PMC article.
-
Intrauterine insemination versus fallopian tube sperm perfusion for non tubal infertility.Cochrane Database Syst Rev. 2004;(3):CD001502. doi: 10.1002/14651858.CD001502.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2009 Apr 15;(2):CD001502. doi: 10.1002/14651858.CD001502.pub3. PMID: 15266448 Updated.
References
-
- Bataille P, Reynard A, Ducarme G. Spontaneous heterotopic triplets – a review of literature. J Gynecol Obstet Hum Reprod. 2017;46:657–9. - PubMed
-
- Maaita ME, Murad N, Dabbas M. Advanced heterotopic pregnancy. J Obstet Gynaecol. 1999;19:677–8. - PubMed
-
- Hewlett K, Howell CM. Heterotopic pregnancy: simultaneous viable and nonviable pregnancies. JAAPA. 2020;33:35–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
