

Early vs. deferred catheter ablation of ventricular tachycardia in patients of ischaemic substrate: systematic review and meta-analysis of clinical outcomes
- PMID: 40630260
- PMCID: PMC12236160
- DOI: 10.1093/ehjopen/oeaf076
Early vs. deferred catheter ablation of ventricular tachycardia in patients of ischaemic substrate: systematic review and meta-analysis of clinical outcomes
Abstract
Aims: Ventricular tachycardia (VT) ablation has been shown to reduce the recurrence of VT episodes, but the timing of performing VT ablation (early; at the time of implantable cardioverter defibrillator implantation) or (deferred: after the patient has received ICD shocks) remains controversial. The objective is to conduct a systematic review and meta-analysis of published data from randomized controlled trials (RCTs) in patients with ischaemic cardiomyopathy (ICM) with the aim of comparing outcome of VT ablation stratified by procedural timing.
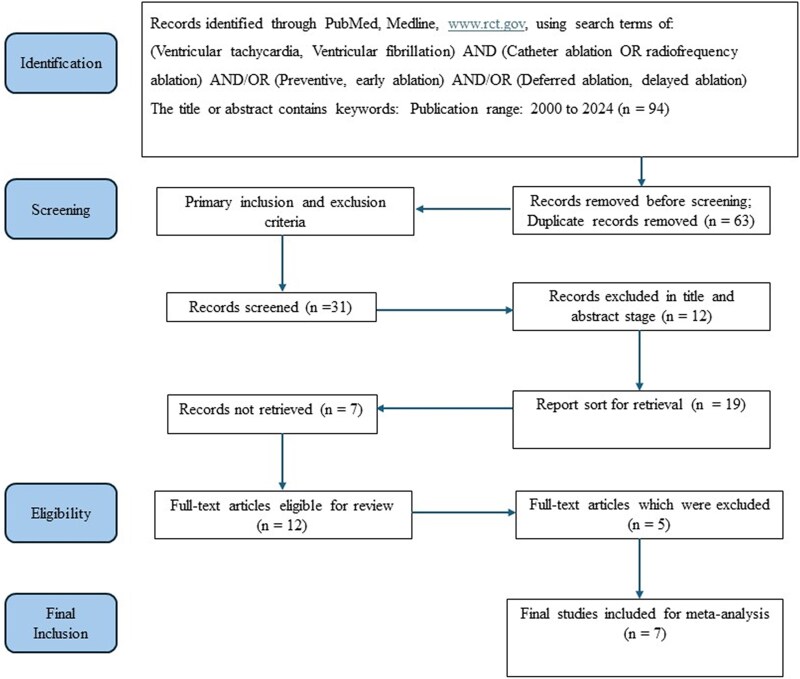
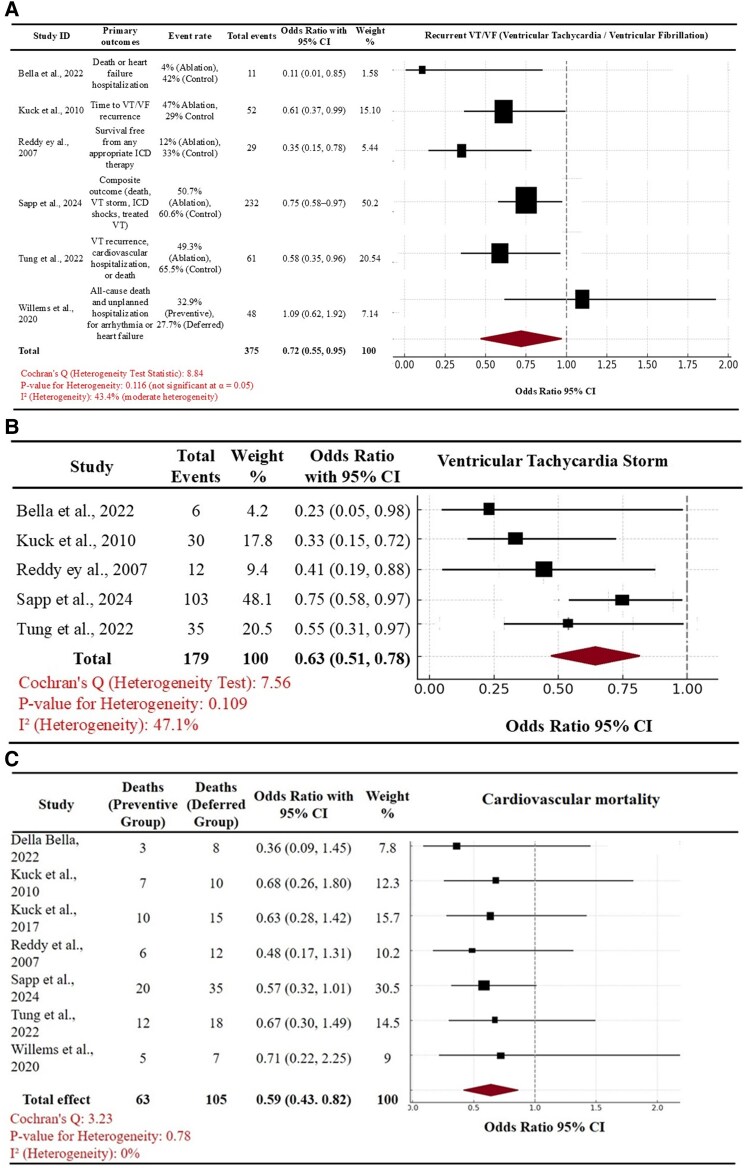
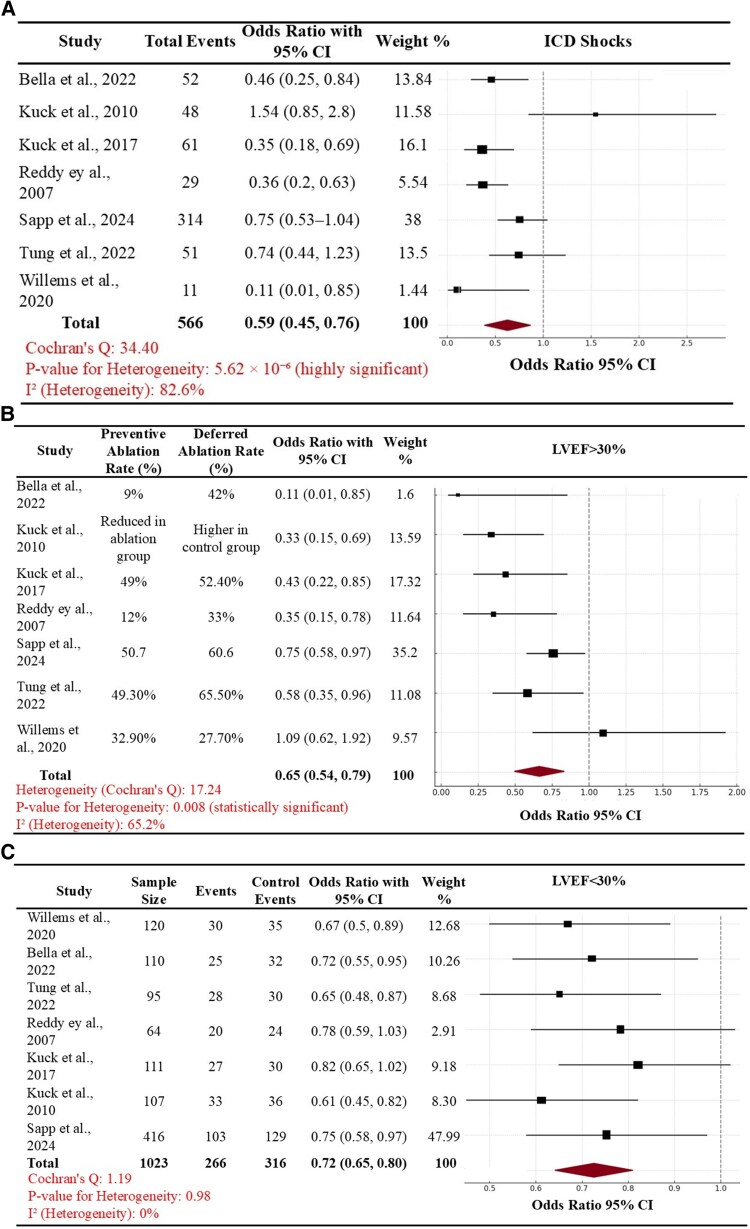
Methods and results: We conducted a meta-analysis of seven landmark RCTs which included patients with ICM who were either at a high risk of VT or experienced VT/ICD shocks. The primary outcome of VT recurrence was compared according to the timing of performing VT ablation (early vs. deferred). In addition, we also compared the secondary outcome of cardiac mortality. Following a comprehensive search strategy, a total of seven RCTs were included within the final analysis. Based on a pooled analysis, early VT ablation was associated with a significant reduction in the primary outcome [pooled odds ratio (OR) of 0.72, 95% confidence interval (CI): 0.55-0.95, P < 0.05] in comparison with a 'deferred VT ablation' strategy. The cumulative absolute risk reduction (ARR) for the primary outcome was 0.21, and number needed to treat (NNT) to prevent the outcome of VT recurrence was 4.81. Furthermore, the effect size of early VT ablation compared to a deferred VT ablation approach was more pronounced in reduction of ICD shocks in the subgroup of patients with LVEF > 30% vs. those with LVEF < 30% (pooled OR of 0.65, 95% CI of 0.54-0.79, P = 0.01). For the secondary outcomes, we observed that an earlier timing of VT ablation was also associated with both a decrease in cardiac mortality (pooled OR of 0.59, 95% CI of 0.43-0.82) and in the subsequent risk of VT storm (pooled OR of 0.63, 95% CI of 0.51-0.78) when compared with a deferred timing. The cumulative ARR for cardiac mortality was 0.07 and NNT was 15.
Conclusion: The findings from this pooled analysis of seven major RCTs suggest that performing early VT ablation may be beneficial in reducing recurrent VT, ICD shocks, and electrical storm and could also improve cardiac mortality. The benefit of performing early VT ablation was greater in patients with LVEF of >30% amongst this ICM cohort.
Keywords: Catheter ablation; Ventricular tachycardia.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Comment on
-
Cardiac function after catheter ablation of ventricular arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy.Eur Heart J Open. 2025 May 5;5(3):oeaf049. doi: 10.1093/ehjopen/oeaf049. eCollection 2025 May. Eur Heart J Open. 2025. PMID: 40458289 Free PMC article.
Similar articles
-
Catheter ablation for ventricular tachycardia (VT) in patients with ischemic heart disease: a systematic review and a meta-analysis of randomized controlled trials.J Interv Card Electrophysiol. 2016 Mar;45(2):111-7. doi: 10.1007/s10840-015-0083-4. Epub 2015 Dec 22. J Interv Card Electrophysiol. 2016. PMID: 26695501
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Catheter ablation versus medical therapy for ventricular tachycardia in patients with ischemic heart disease: A systematic review and meta-analysis of randomized controlled trials.Indian Pacing Electrophysiol J. 2025 Mar-Apr;25(2):91-103. doi: 10.1016/j.ipej.2025.03.004. Epub 2025 Mar 7. Indian Pacing Electrophysiol J. 2025. PMID: 40058526 Free PMC article.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost-utility for these groups in a UK context.Health Technol Assess. 2006 Aug;10(27):iii-iv, ix-xi, 1-164. doi: 10.3310/hta10270. Health Technol Assess. 2006. PMID: 16904046
References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, Charron P, Corrado D, Dagres N, de Chillou C, Eckardt L, Friede T, Haugaa KH, Hocini M, Lambiase PD, Marijon E, Merino JL, Peichl P, Priori SG, Reichlin T, Schulz-Menger J, Sticherling C, Tzeis S, Verstrael A, Volterrani M; ESC Scientific Document Group . 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Winterfield JR, Kent AR, Karst E, Dalal N, Mahapatra S, Bunch TJ, Reynolds MR, Wilber DJ. Impact of ventricular tachycardia ablation on health care utilization. Heart Rhythm 2018;15:355–362. - PubMed
-
- Wathen MS, DeGroot PJ, Sweeney MO, Stark AJ, Otterness MF, Adkisson WO, Canby RC, Khalighi K, Machado C, Rubenstein DS, Volosin KJ; PainFREE Rx II Investigators . Prospective randomized multicenter trial of empirical antitachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter-defibrillators: pacing fast ventricular tachycardia reduces shock therapies (PainFREE Rx II) trial results. Circulation 2004;110:2591–2596. - PubMed
-
- Kheiri B, Barbarawi M, Zayed Y, Hicks M, Osman M, Rashdan L, Kyi HH, Bachuwa G, Hassan M, Stecker EC, Nazer B, Bhatt DL. Antiarrhythmic drugs or catheter ablation in the management of ventricular tachyarrhythmias in patients with implantable cardioverter defibrillators: a systematic review and meta-analysis of randomized controlled trials. Circ Arrhythm Electrophysiol 2019;12:e007600. - PubMed
-
- Samuel M, Healey JS, Nault I, Sterns LD, Essebag V, Gray C, Hruczkowski T, Gardner M, Parkash R, Sapp JL. Ventricular tachycardia and ICD therapy burden with catheter ablation versus escalated antiarrhythmic drug therapy. JACC Clin Electrophysiol 2023;9:808–821. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
