

Diagnostic Value of Biological Parameters in Biopsy-Confirmed Thrombotic Microangiopathy-MATRIX Consortium Group
- PMID: 40630316
- PMCID: PMC12232970
- DOI: 10.1016/j.ekir.2025.03.019
Diagnostic Value of Biological Parameters in Biopsy-Confirmed Thrombotic Microangiopathy-MATRIX Consortium Group
Abstract
Introduction: The diagnosis of thrombotic microangiopathy (TMA) relies on common biological parameters, the diagnostic value of which are unknown.
Methods: The presence of common biological parameters was assessed in 967 patients with TMA from 2009 to 2023 (ClinicalTrials.gov: NCT05991245).
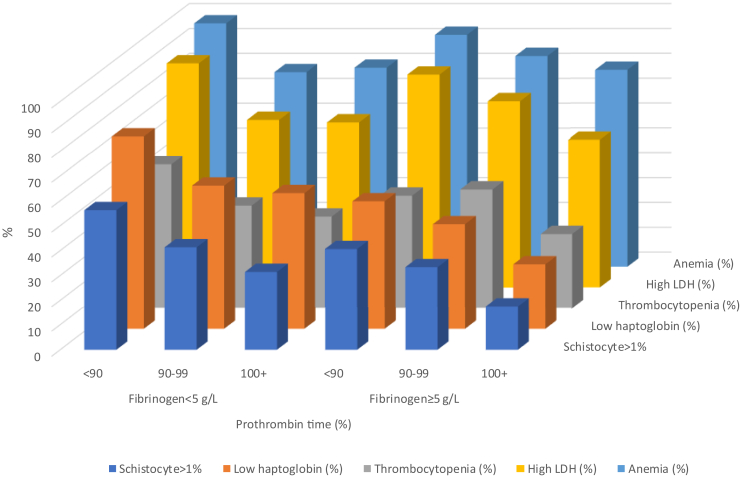
Results: The median age was 49 (36-64) years and 53.2% were male. All TMA causes were represented (atypical hemolytic uremic syndrome [aHUS]: 41.6%, drugs: 24.9%, malignancy: 21.4%, autoimmune disease: 18.8%, infection: 7.6%, complement-mediated HUS: 6.8%, organ transplantation: 5.8%, pregnancy: 3.8%, bone marrow transplantation [BMT]: 2.9%, Shiga toxin Escherichia coli hemolytic uremic syndrome [STEC-HUS]: 0.6%, and thrombotic thrombocytopenic purpura [TTP]: 0.6%). The presence of TMA-related parameters concerned virtually all patients with TTP but varied widely for the other patients as follows: anemia: 81.7%, high lactate dehydrogenase (LDH) (75.4%), low haptoglobin (53.7%), and thrombocytopenia (40.3%). Their diagnostic performance was accurate only for TTP. Eleven distinct ways were used for schistocyte metrics and reporting. Relying on schistocyte presence as the single diagnostic criterion would lead to missed diagnosis in 23.8% (STEC-HUS) to 86.4% (BMT) of patients (for anemia: 8.2%-22.3%; thrombocytopenia: 31.8%-67.9%; high LDH: 10.0%-40.7%, low haptoglobin: 0%-70.4%, according to the causes of TMA). The overall risk of missed diagnosis using these parameters was ≥ 50% in all TMA, except in TTP. The best diagnostic performances were obtained when fibrinogen levels were < 5 g/l, creatinine ≥ 300 μmol/l, prothrombin time (PT) < 90%; and when TMA causes were TTP, STEC-HUS, infection, or complement-mediated HUS.
Conclusion: Common biological parameters miss the diagnosis in more than 50% of TMA except when fibrinogen is < 5 g/l, creatinine ≥ 300 μmol/l, and PT < 90%. Schistocyte reporting is heterogenous, and its results are usually deceptive in TMA.
Keywords: biological parameters; cohort; schistocytes; thrombotic microangiopathy.
© 2025 International Society of Nephrology. Published by Elsevier Inc.
Figures


References
Associated data
LinkOut - more resources
Full Text Sources
Medical
