

Final analysis of the ZOE-LTFU trial to 11 years post-vaccination: efficacy of the adjuvanted recombinant zoster vaccine against herpes zoster and related complications
- PMID: 40630610
- PMCID: PMC12235393
- DOI: 10.1016/j.eclinm.2025.103241
Final analysis of the ZOE-LTFU trial to 11 years post-vaccination: efficacy of the adjuvanted recombinant zoster vaccine against herpes zoster and related complications
Abstract
Background: Herpes zoster (HZ) vaccines should provide durable protection against HZ and HZ-related complications. We report the final analysis of a long-term follow-up (LTFU) study (ZOE-LTFU) including 11 years of follow-up after primary vaccination with recombinant zoster vaccine (RZV).
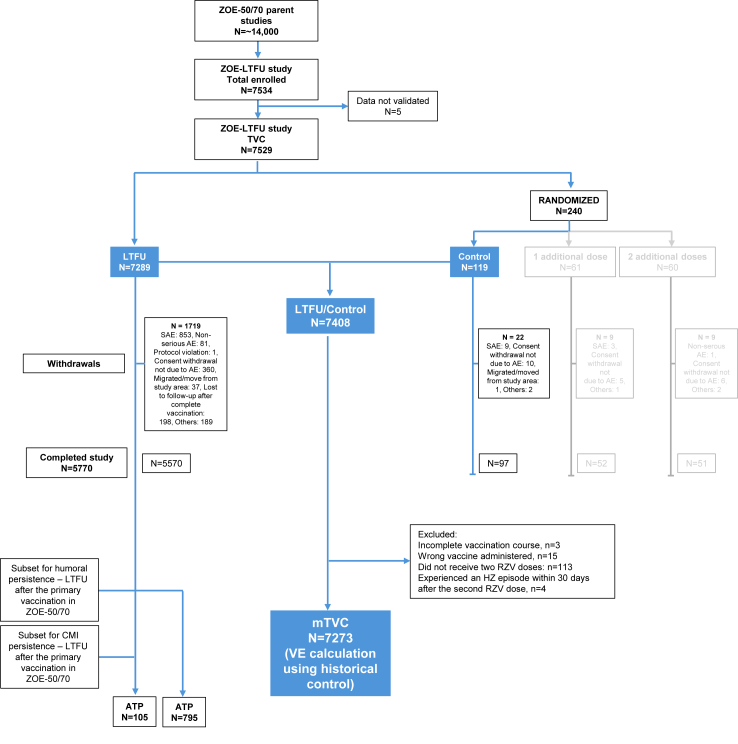
Methods: ZOE-LTFU (NCT02723773) was an open-label, phase 3b study following participants of two phase 3 trials, ZOE-50 and ZOE-70. ZOE-LTFU started approximately 5 years post-vaccination in ZOE-50/70 and participants were followed for 6 years. The primary objective was to assess vaccine efficacy (VE) against HZ during ZOE-LTFU. Secondary objectives included VE against HZ from 1 month post-dose 2 in ZOE-50/70 until end of ZOE-LTFU, VE against post-herpetic neuralgia (PHN) and non-PHN complications, immunogenicity, and long-term safety. The VE calculation used a historical control constructed with ZOE-50/70 placebo data.
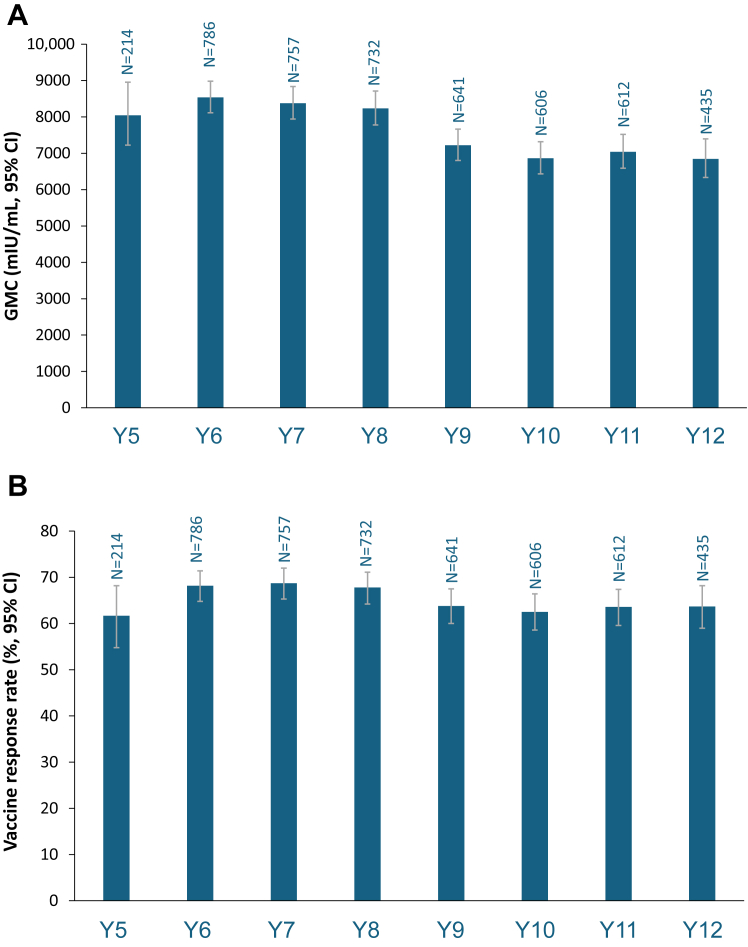
Findings: VE was assessed in the modified total vaccinated cohort (n = 7273 [mean age 67·3 years at first vaccination]). During ZOE-LTFU, VE was 79·8% (95% confidence interval [CI]: 73·7, 84·6) and 73·2% (95% CI: 62·9, 80·9) against HZ in participants ≥50 and ≥70 years at first vaccination, respectively, and was 87·5% (95% CI: 64·8, 96·8) against PHN and 91·7% (95% CI: 43·7, 99·8) against other HZ-related complications in participants ≥50 years. From 1 month post-dose 2 in ZOE-50/70 to the end of ZOE-LTFU, VE against HZ was 87·7% (95% CI: 84·9, 90·1) in participants ≥50 years and sustained at 82·0% (95% CI: 63·0, 92·2) in the eleventh year post-vaccination. Humoural and cell-mediated immune responses plateaued at over 5-fold and ∼7-fold, respectively, above pre-vaccination levels in ZOE-50/70. No RZV-related serious adverse events occurred.
Interpretation: Efficacy of RZV against HZ and associated complications remained high through 11 years post-vaccination, indicating sustained clinical benefit.
Funding: The funder of the study was GSK who was involved in study design, data collection, data analysis, data interpretation, writing of the report, and the decision to submit for publication.
Keywords: Herpes zoster; Long-term follow-up; Post-herpetic neuralgia; Recombinant zoster vaccine.
© 2025 GSK plc.
Conflict of interest statement
Ana Strezova is employed by GSK and holds financial equities in GSK. Javier Díez Domingo reports payments to his institution from GSK, Sanofi, MSD, Moderna, and AZ sponsored studies. Javier Díez Domingo also reports payments from GSK, Sanofi Pasteur, Pfizer, and Moderna, as well as support for attending meetings and/or travel from GSK and Pfizer. Anthony L Cunningham reports payments to his institution from GSK, Moderna, Seqirus, Abbvie, and Healthed. Anthony L Cunningham also reports support for attending meetings and/or travel from GSK and Moderna. Takashi Eto declares no financial and non-financial relationships and activities and no conflicts of interest. Charles Andrews reports consulting fees from Boehringer Ingelheim, Merck, and Bayer, as well as participation on boards for Moderna. Clovis Arns reports honoraria for lectures and presentations, and payments for attending meetings and/or travel from GSK. Eun-Ju Choo declares no financial and non-financial relationships and activities and no conflicts of interest. David Shu Cheong Hui declares no financial and non-financial relationships and activities and no conflicts of interest. Giancarlo Icardi declares no financial and non-financial relationships and activities and no conflicts of interest. Shelly A McNeil reports payments to her institution from GSK and consulting fees or participation on advisory boards and a DSMB from GSK. Airi Põder declares no financial and non-financial relationships and activities and no conflicts of interest. Pavel Kosina declares no financial and non-financial relationships and activities and no conflicts of interest. Lars Rombo declares no financial and non-financial relationships and activities and no conflicts of interest. Tino F Schwarz reports payments from AstraZeneca, Bavarian Nordic, Biogen, Biontech, CRM, CSL Seqirus, CSL Vifor, GSK, Janssen-Cilag, Merck-Serono, Moderna, Novavax, MSD, Pfizer, Roche, Sanofi-Aventis, Synlab, Takeda. Tino F Schwarz also reports participantions on boards for Bavarian Nordic, Biontech, CSL Seqirus, GSK, Moderna, Novavax, Takeda. Juan Carlos Tinoco reports payments for lectures and speakers bureaus from GSK. Chong-Jen Yu declares no financial and non-financial relationships and activities and no conflicts of interest. Jing Wang is employed by GSK. Jyoti Soni is employed by GSK and holds financial equities in GSK. Manyee Tsang is employed by GSK and holds financial equities in GSK. Rafael Leon is employed by GSK and holds financial equities in GSK. Agnes Mwakingwe-Omari is employed by GSK and holds financial equities in GSK. The authors declare no other financial and non-financial relationships and activities.
Figures



References
-
- Oxman M.N. Herpes zoster pathogenesis and cell-mediated immunity and immunosenescence. J Am Osteopath Assoc. 2009;109(6 Suppl 2):S13–S17. - PubMed
-
- Dworkin R.H., Johnson R.W., Breuer J., et al. Recommendations for the management of herpes zoster. Clin Infect Dis. 2007;44(Suppl 1):S1–S26. - PubMed
-
- Centers for Disease Control and Prevention Clinical features of shingles (herpes zoster) 2024. https://www.cdc.gov/shingles/hcp/clinical-signs/index.html
LinkOut - more resources
Full Text Sources
