

Lumbosacral Vertebral Angles can Predict Lumbosacral Transitional Vertebrae on Routine Sagittal MRI
- PMID: 40630817
- PMCID: PMC12232574
- DOI: 10.22038/ABJS.2025.83244.3790
Lumbosacral Vertebral Angles can Predict Lumbosacral Transitional Vertebrae on Routine Sagittal MRI
Abstract
Objectives: We aimed to measure lumbosacral vertebral angles in routine lumbar sagittal MRIs and assess their association with lumbosacral transitional vertebrae (LSTV).
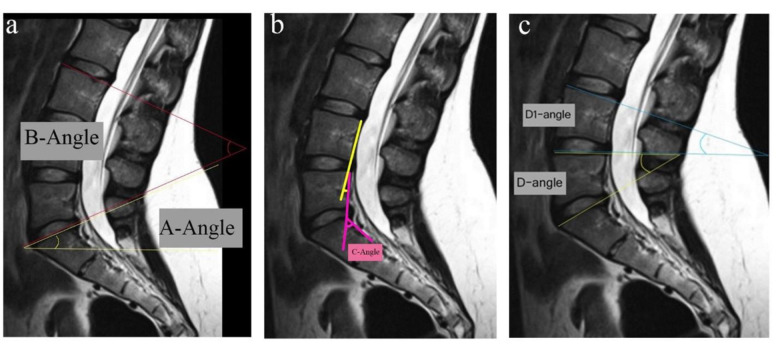
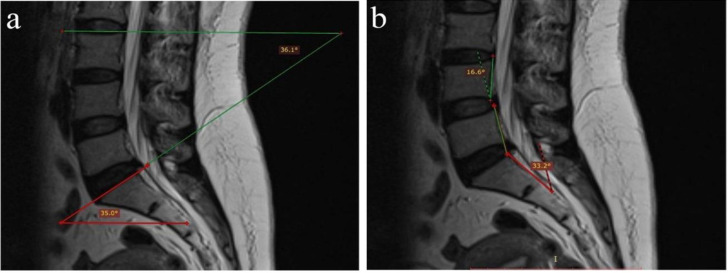
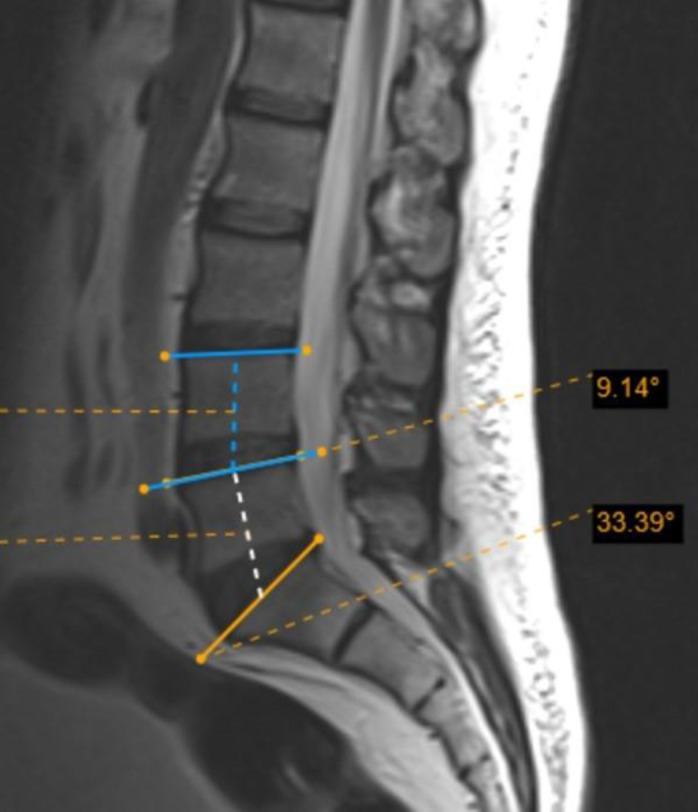
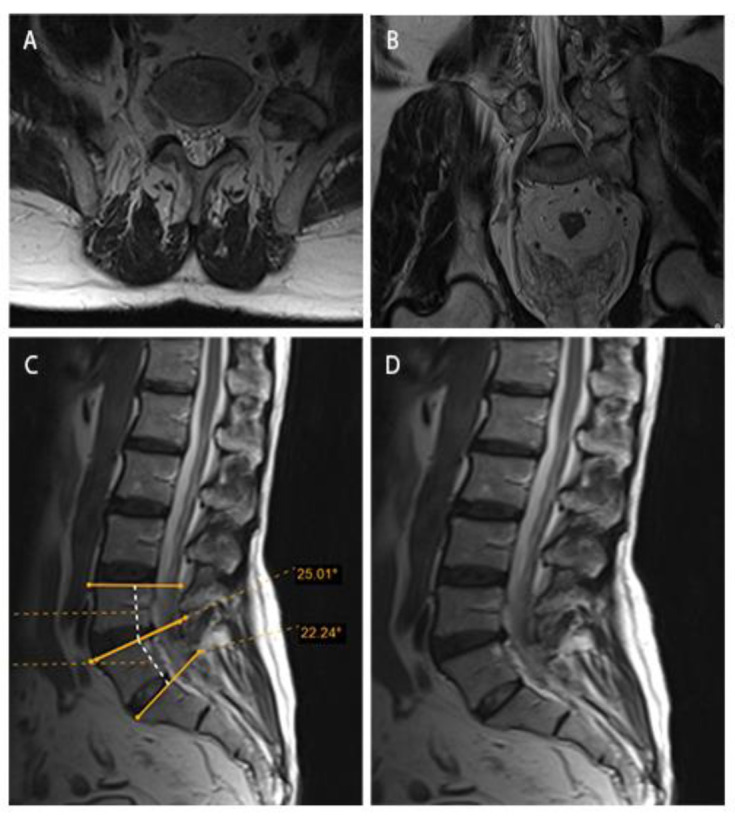
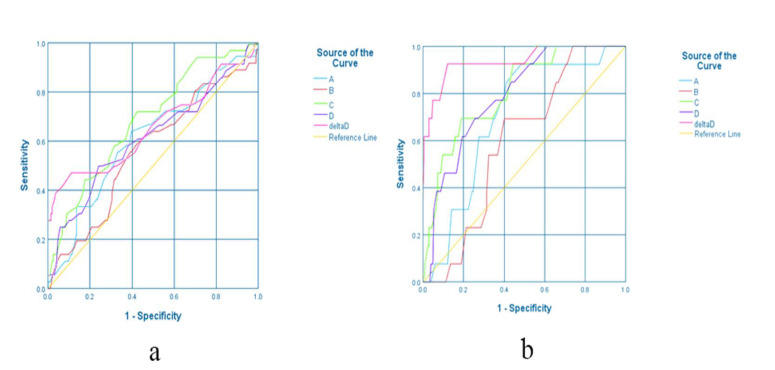
Methods: We recruited 220 patients referring to our hospital for routine lumbar MRI during 2020-2021. All the participants were subject to routine sagittal lumbar MRI, whole spine localizer scan, and coronal MRI to numerate lumbar vertebrae. Five vertebral angles (A, B, C, D, and delta) and dehydration in L4-L5 and L5-S1 discs were assessed in sagittal MRI scans. Data were analyzed using SPSS 26.
Results: Out of 220 participants (mean age: 44.29 ± 14.14 years), 36 (16.36%) were diagnosed with LSTV. Among those diagnosed with LSTV, L5-S1 dehydration was less frequently observed compared to other participants (P < 0.001). Multivariate regression showed that dehydrated L4-L5 disc, non-dehydrated L5-S1 disc, increased A-angle, and decreased D-angle can independently predict LSTV. The median A-angle was significantly larger in LSTV patients than in non-LSTV participants (P = 0.038), while the medians of C-angle, D-angle, and delta-angle were significantly smaller in the LSTV group (P < 0.05). A C-angle ≤ 35.5˚ could diagnose LSTV with sensitivity and specificity of 72.2% and 57.6%, respectively. A delta angle ≤ 8.5˚ could diagnose type 2 LSTV with 92.3% sensitivity and 87.9% specificity.
Conclusion: Measuring lumbosacral vertebral angles, especially delta-angle, in routine sagittal MRI can potentially alert physicians of a likely LSTV diagnosis.
Keywords: Angle; Diagnosis; Lumbosacral transitional vertebrae; Magnetic resonance imaging.
© 2025 Mashhad University of Medical Sciences.
Conflict of interest statement
The authors do NOT have any potential conflicts of interest for this manuscript.
Figures
Similar articles
-
The Implications of Sacralized Transitional Vertebra on Spinal Alignment.Spine (Phila Pa 1976). 2025 Aug 1;50(15):1081-1089. doi: 10.1097/BRS.0000000000005187. Epub 2024 Oct 15. Spine (Phila Pa 1976). 2025. PMID: 39451150
-
Lumbosacral transitional vertebra alters the mobility of the lumbar spine on flexion-extension radiographs.Int Orthop. 2025 Aug 13. doi: 10.1007/s00264-025-06637-7. Online ahead of print. Int Orthop. 2025. PMID: 40801985
-
Paraspinal Muscle Alterations in Lumbosacral Transitional Vertebrae: A Volumetric Study of Low Back Pain Patients.Acad Radiol. 2025 Jun 26:S1076-6332(25)00560-4. doi: 10.1016/j.acra.2025.06.012. Online ahead of print. Acad Radiol. 2025. PMID: 40579255
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Castellvi AE, Goldstein LA, Chan DP. Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Spine (Phila Pa 1976) 1984;9(5):493–5. - PubMed
-
- Hanhivaara J, Määttä JH, Karppinen J, Niinimäki J, Nevalainen MT. The association of lumbosacral transitional vertebrae with low back pain and lumbar degenerative findings in MRI: a large cohort study. Spine (Phila Pa 1976) 2022;47(2):153–162. - PubMed
-
- Hsieh CY, Vanderford JD, Moreau SR, Prong T. Lumbosacral transitional segments: classification, prevalence, and effect on disk height. J Manipulative Physiol Ther. 2000;23(7):483–9. - PubMed
-
- Otani K, Konno S, Kikuchi S. Lumbosacral transitional vertebrae and nerve-root symptoms. J Bone Joint Surg Br. 2001;83(8):1137–40. - PubMed
-
- Jenkins III AL, Chung RJ, O’Donnell J, et al. Redefining the treatment of lumbosacral transitional vertebrae for Bertolotti syndrome: Long-term outcomes utilizing the Jenkins classification to determine treatment. World Neurosurg. 2023;175: e21–e29. - PubMed
LinkOut - more resources
Full Text Sources