

Individual Risk Assessment and Prognostication of Outcomes After Corneal Cross-Linking
- PMID: 40630907
- PMCID: PMC12237562
- DOI: 10.1155/joph/3678453
Individual Risk Assessment and Prognostication of Outcomes After Corneal Cross-Linking
Abstract
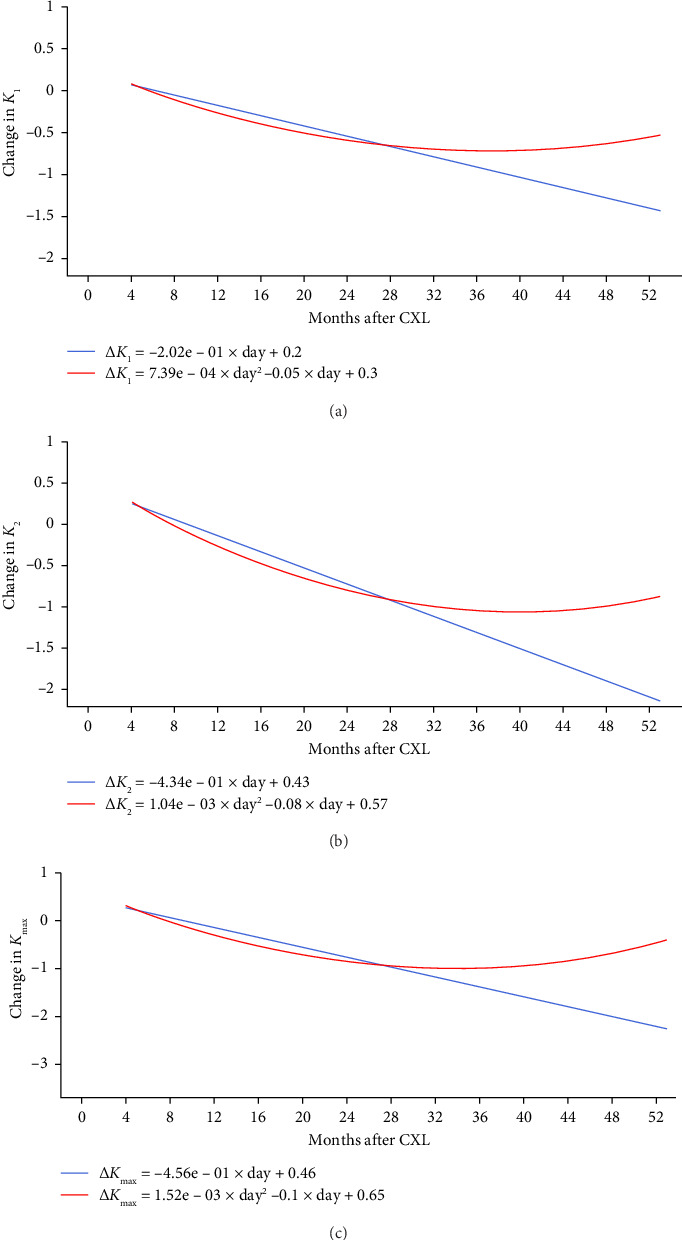
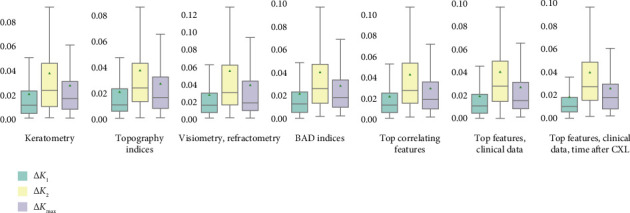
Background and Objective: Corneal collagen cross-linking (CXL) is a treatment which arrests keratoconus (KC) progression, but its effectiveness differs radically among patients. Herein, we report preoperative diagnostic findings that reflect CXL outcomes and allow physicians to prognosticate treatment efficiency. Methods: In a medical centre, we retrospectively analysed pre- and postoperative data about 107 patients (112 eyes) treated with CXL from January 2018 to December 2022. Exclusion criteria were age below 16 years, a corneal thickness below 400 microns, severe dry eye, other corneal diseases/infections, re-CXL, pregnancy and missing follow-up examinations. All the subjects (79 males and 28 females) were followed for a minimum of 4 and a maximum of 40 months. The study dataset was comprised of 796 cases of clinical assessment, pachymetry, visiometry, refractometry and topography examinations. With these data, we modelled maximum anterior keratometry (K max) and curvature power of the flat and steep meridians of the corneal anterior surface (K 1 and K 2). Results: Two years after the invasion, corneal curvature coefficients decreased progressively. Then, they remained stable for four months and rose afterwards. In the most accurate K 1, K 2 and K max models, the proportion of mean absolute error to the range of values was 1.72, 3.66 and 2.37%, respectively. Pronounced corneal thinning, low best-corrected visual acuity and high K max levels predict unfavourable outcomes. Conclusions: The high accuracy of the models advocates for a personalised approach to candidate selection for CXL.
Keywords: corneal collagen cross-linking; explainable artificial intelligence; intervention outcome; keratoconus; keratometry readings; machine learning; precision medicine; predictive model.
Copyright © 2025 Y. Statsenko et al. Journal of Ophthalmology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interests.
Figures

References
LinkOut - more resources
Full Text Sources
