

Association Between COVID-19 During Pregnancy and Preterm Birth by Trimester of Infection: Retrospective Cohort Study Using Large-Scale Social Media Data
- PMID: 40632790
- PMCID: PMC12266298
- DOI: 10.2196/66097
Association Between COVID-19 During Pregnancy and Preterm Birth by Trimester of Infection: Retrospective Cohort Study Using Large-Scale Social Media Data
Abstract
Background: Preterm birth, defined as birth at <37 weeks of gestation, is the leading cause of neonatal death globally and the second leading cause of infant mortality in the United States. There is mounting evidence that COVID-19 infection during pregnancy is associated with an increased risk of preterm birth; however, data remain limited by trimester of infection. The ability to study COVID-19 infection during the earlier stages of pregnancy has been limited by available sources of data.
Objective: The objective of this study was to use self-reports in large-scale social media data to assess the association between the trimester of COVID-19 infection and preterm birth.
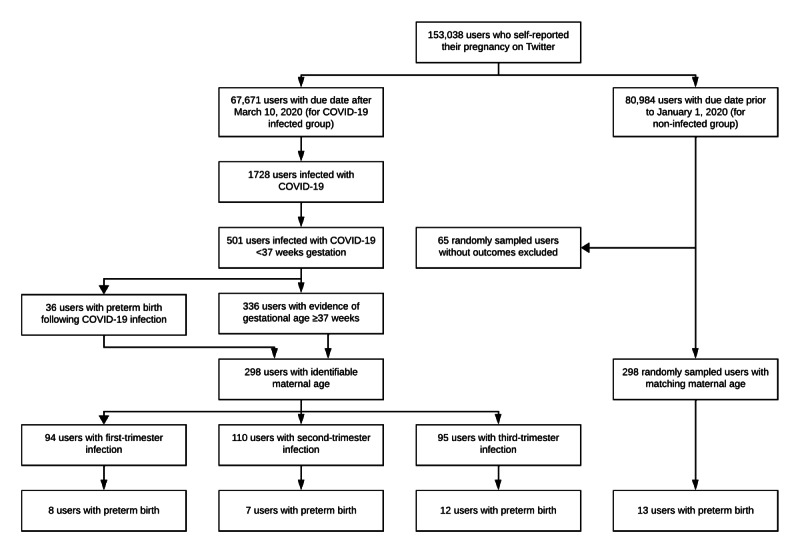
Methods: In this retrospective cohort study, we used natural language processing and machine learning, followed by manual validation, to identify self-reports of pregnancy on Twitter and to search these users' collection of publicly available tweets for self-reports of COVID-19 infection during pregnancy and, subsequently, a preterm birth or term birth outcome. Among the users who reported their pregnancy on Twitter, we also identified a 1:1 age-matched control group, consisting of users with a due date before January 1, 2020-that is, without COVID-19 infection during pregnancy. We calculated the odds ratios (ORs) with 95% CIs to compare the frequency of preterm birth for pregnancies with and without COVID-19 infection and by the timing of infection: first trimester (1-13 weeks), second trimester (14-27 weeks), or third trimester (28-36 weeks).
Results: Through August 2022, we identified 298 Twitter users who reported COVID-19 infection during pregnancy, a preterm birth or term birth outcome, and maternal age: 94 (31.5%) with first-trimester infection, 110 (36.9%) with second-trimester infection, and 95 (31.9%) with third-trimester infection. In total, 26 (8.8%) of these 298 users reported preterm birth: 8 (8.5%) with first-trimester infection, 7 (6.4%) with second-trimester infection, and 12 (12.6%) with third-trimester infection. In the 1:1 age-matched control group, 13 (4.4%) of the 298 users reported preterm birth. Overall, the odds of preterm birth were significantly higher for pregnancies with COVID-19 infection compared to those without (OR 2.08, 95% CI 1.06-4.28; P=.046). In particular, the odds of preterm birth were significantly higher for pregnancies with COVID-19 infection during the third trimester (OR 3.16, 95% CI 1.36-7.29; P=.007). The odds of preterm birth were not significantly higher for pregnancies with COVID-19 infection during the first trimester (OR 2.05, 95% CI 0.78-5.08; P=.12) or second trimester (OR 1.50, 95% CI 0.54-3.82; P=.44) compared to those without infection.
Conclusions: Based on self-reports in large-scale social media data, the results of our study suggest that COVID-19 infection particularly during the third trimester is associated with higher odds of preterm birth.
Keywords: COVID-19; epidemiology; machine learning; natural language processing; pregnancy; preterm birth; social media.
© Ari Z Klein, Shriya Kunatharaju, Su Golder, Lisa D Levine, Jane C Figueiredo, Graciela Gonzalez-Hernandez. Originally published in the Journal of Medical Internet Research (https://www.jmir.org).
Conflict of interest statement
Update of
-
Association Between COVID-19 During Pregnancy and Preterm Birth by Trimester of Infection: A Retrospective Cohort Study Using Longitudinal Social Media Data.medRxiv [Preprint]. 2023 Nov 21:2023.11.17.23298696. doi: 10.1101/2023.11.17.23298696. medRxiv. 2023. Update in: J Med Internet Res. 2025 Jul 9;27:e66097. doi: 10.2196/66097. PMID: 38045356 Free PMC article. Updated. Preprint.
Similar articles
-
Association Between COVID-19 During Pregnancy and Preterm Birth by Trimester of Infection: A Retrospective Cohort Study Using Longitudinal Social Media Data.medRxiv [Preprint]. 2023 Nov 21:2023.11.17.23298696. doi: 10.1101/2023.11.17.23298696. medRxiv. 2023. Update in: J Med Internet Res. 2025 Jul 9;27:e66097. doi: 10.2196/66097. PMID: 38045356 Free PMC article. Updated. Preprint.
-
Safety of SARS-CoV-2 vaccination during pregnancy- obstetric outcomes from a large cohort study.BMC Pregnancy Childbirth. 2022 Feb 28;22(1):166. doi: 10.1186/s12884-022-04505-5. BMC Pregnancy Childbirth. 2022. PMID: 35227233 Free PMC article.
-
Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD003510. doi: 10.1002/14651858.CD003510.pub3. Cochrane Database Syst Rev. 2011. PMID: 21735394
-
Multiple-micronutrient supplementation for women during pregnancy.Cochrane Database Syst Rev. 2017 Apr 13;4(4):CD004905. doi: 10.1002/14651858.CD004905.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2019 Mar 14;3:CD004905. doi: 10.1002/14651858.CD004905.pub6. PMID: 28407219 Free PMC article. Updated.
-
Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection.Cochrane Database Syst Rev. 2007 Jan 24;(1):CD003510. doi: 10.1002/14651858.CD003510.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2011 Jul 06;(7):CD003510. doi: 10.1002/14651858.CD003510.pub3. PMID: 17253490 Updated.
References
-
- Murphy SL, Kochanek KD, Xu J, et al. Mortality in the United States, 2020. NCHS Data Brief. 2021 Dec;427(427):1–8. Medline. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
